Volz S. Eur Heart J. 2021 Jul 15;42(27):2657-2664.
In addition to optimal medical therapy (OMT), American guidelines recommend an intrusive process in patients with decreased left ventricular ejection fraction (LVEF) and multivessel disease (MVD). Randomized controlled trials in these patients have demonstrated that long-term survival is higher after coronary artery bypass grafting (CABG) as compared to OMT alone. But, the impacts of percutaneous coronary intervention (PCI) in patients with HF and concomitant MVD have not been assessed in a randomized setting. Thus, Volz S, et al. conducted a study to analyse the correlation among CABG vs. PCI and mortality in a national group of patients with HF and concomitant MVD.
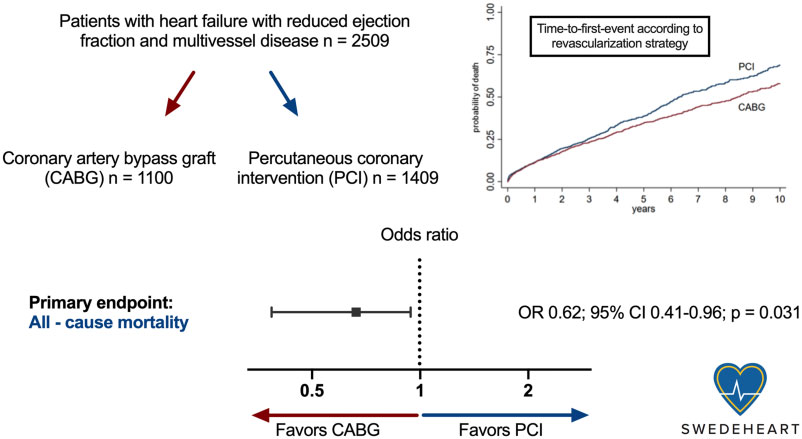
Patients with heart failure with reduced ejection fraction and multivessel disease (coronary artery stenosis >50% in ≥2 vessels or left main) who underwent coronary angiography between 2000 and 2018 in Sweden were enrolled in the study. An all-cause mortality was assessed after CABG or PCI in these patients. A propensity score-adjusted logistic and Cox proportional-hazards regressions and instrumental variable model were used to adjust for known and unknown confounders. Multilevel modelling was utilized to adjust for the arraying of examinations in a hierarchical database. The primary endpoint was all-cause mortality
Total 2509 patients [2080 (82.9%) men and 429 (17.1%) women] were incorporated in the study; 35.8% showed diabetes, and 34.7% showed a previous myocardial infarction. The mean age was 68.1± 9.4 years (47.8% were >70 years old), and 64.9% showed three-vessel or left main disease. The primary designated therapy following coronary angiography was PCI in 1409 (56.2%) and CABG in 1100 (43.8%) individuals. Median follow-up time was 3.9 years (range 1 day to 10 years).
Across the study period, there were 1010 (40.5%) patients had deaths. Coronary artery bypass grafting was correlated with a lower risk of death than PCI [odds ratio (OR) 0.62; 95% CI 0.41–0.96; p= 0.031] (Figure 1).
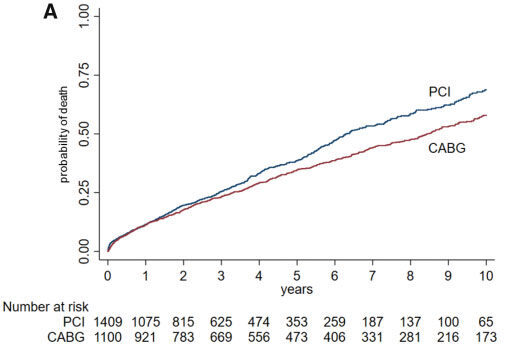
Figure 1: Time-to-first-event curves for all-cause mortality through 10-year follow-up.
Survival curves start separating after the 3rd year. Given non-proportional hazards during the follow-up period, logistic regression with follow-up time included as a log-transformed offset variable was used to calculate the odds ratios with 95% confidence intervals as a primary analysis.
We found substantial impact modification among diabetes and CABG (pinteraction = 0.041). There was no interaction among the revascularization method and age, sex, calendar year, and the severity of coronary artery disease (Figure 2). The risk of death elevated (OR 1.27, 95% CI 1.17–1.38, ptrend < 0.001) directly with quintiles of hospitals in which PCI was the preferred procedure for revascularization.
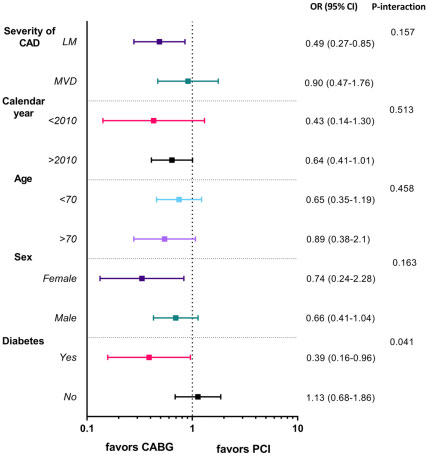
Figure 2: Subgroup analysis for all-cause mortality.
Quantitative interaction between diabetes and coronary artery bypass grafting (p = 0.041)
Graphical abstract
Patients with ischaemic HF, CABG was correlated with better long-term survival as compared to PCI. This result was supported by centre-level data exhibiting that tendency towards executing PCI rather than CABG was correlated with an inferior auguring. But, PCI is still the preferred revascularization procedure in the most of Swedish hospitals in these patients. Study assists the current European and American guidelines for revascularization of patients with HF because of ischaemic heart disease. There is a requirement for a randomized trial to determine the question of which revascularization procedure should be the therapy of choice in patients with ischaemic HF.
