Extracorporeal Cardiopulmonary Resuscitation for Refractory Out of Hospital Cardiac Arrest (EROCA) – Results of a Randomized Feasibility Trial of Expedited Prehospital Transport
Extracorporeal cardiopulmonary resuscitation (ECPR) for out-of-hospital cardiac arrest (OHCA) is auspicious however is unproven, and consequences are greatly dependent on time to initiation of treatment. Expedited transport may facilitate opportunities for ECPR in clinical practice and future trials. Meurer WJ, presented a study in a session at American Heart Association Scientific Sessions 2020: A Virtual Experience which hypothesized that a real-time dispatch-based computer algorithm could choose refractory OHCA patients who could be accurately transported to the emergency department (ED) within 30 min of the 911 call, and that Emergency Medicine physicians could begin ECPR in eligible patients within 30 min of ED occurrence. Adults with refractory shockable or witnessed OHCA were randomized 4:1 to expedited transport (ET) or standard prehospital care (SC) in a 2-tiered EMS system serving a US city of 100k in 29 square miles with an ECPR capable primary destination hospital, if the forecasted 911 to ED arrival time was <30 min. A maximum sample size of 24 was arranged. The study needed exception from informed agreement. The primary outcomes were the proportion of patients with 911 to ED arrival <30 min and ED arrival to ECPR flow <30 min.
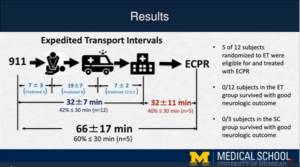
15 participants (10%) from the 156 cardiac arrest runs, were randomized earlier to ending the trial for slow growth. 5 of 12 patients randomized to accelerated transport showed an ED arrival time of <30 min (mean 32.5+7.1). All ECPR eligible patients were cannulated, 3 of 5 receiving ECPR showed initiated flow with <30 min of ED arrival (mean 32.4+10.9), and 7 were ECPR ineligible. 1 patient (randomized to SC) survived to 30 days, and no patients in either group survived with a good neurological consequence.
In an ECPR capable system, EROCA exhibited a functional model for selecting patients with refractory OHCA for ET however did not reach predefined time-interval targets. These results showed significant insight into the increase of ECPR clinical trials and clinical practice based on selected target intervals.
Multicentric, Randomized Controlled Phase III Study of Centhaquine (Lyfaquin®) as an Effective First-in-class Resuscitative Agent in Hypovolemic Shock Patients
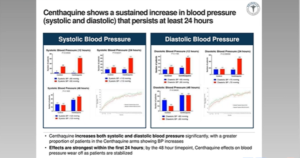
Centhaquine (CQ) is a new, first-in-class resuscitative agent for the management of hypovolemic shock. Gulati A, presented in a session at American Heart Association Scientific Sessions 2020: A Virtual Experience which analysed the effectiveness of CQ as an adjuvant to standard of care (SOC) for the therapy of hypovolemic shock in a prospective, multi-center, randomized, double-blind, placebo-controlled Phase 3 study. Key inclusion criteria were; systolic blood pressure of <90 mmHg, blood lactate levels of > 2 mmol/L and patients acquiring SOC in a hospital or ICU setting. Patients were randomized in a 2:1 ratio either to the CQ group acquiring CQ dose of 0.01 mg/kg by IV infusion along with SOC or to the control group acquiring SOC plus saline. Primary endpoints of the study were change in systolic blood pressure (SBP) and diastolic blood pressure (DBP), change in blood lactate levels and change in base deficit. The key secondary endpoint was mortality via day 28. A total of 197 patients were evaluated, of which 105 patients met the eligibility criteria and were included in the study. 71 patients were randomized to CQ group and 34 patients to control group from the 105 patients. Demographics and baseline characteristics of patients was equivalent in both groups. At the time of inclusion in the study, haemoglobin level was 9.38 ± 0.71 g/dL and 8.73 ± 0.55 g/dL in control and CQ groups, respectively. At 24 hours of resuscitation, 59.38% patients of control group and 81.82% patients of CQ group showed SBP more than 110 mmHg and (p=0.00842). Similarly, 50% patients in control group and 78.46% patients in CQ group showed DBP more than 70 mmHg at 24 hours of resuscitation (p=0.002175). 46.88% patients with standard therapy with blood lactate levels of 1.5 mmol/L or less were compared with 69.35% in CQ group (p=0.0168). The number of patients with base-deficit of less than minus 2 were 46.88% in standard treatment group than 68.25% in those receiving CQ (p=0.0217). CQ treatment substantially decreased the mortality rate. The control group showed the 11.76% mortality rate than 2.94% in the CQ group (odds ratio: 4.4; 95% CI 0.9651 to 23.74 and p=0.037). No drug associated adverse event was described.
Centhaquine (Lyfaquin®) is a greatly effective resuscitative agent for the therapy of hypovolemic shock as an adjuvant to SOC.
Critical Care Management, Hospital Case Volume, and Survival After Extracorporeal Cardiopulmonary Resuscitation
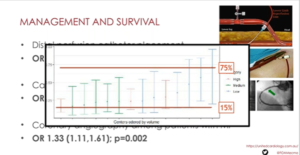
The association among post-resuscitation treatment and survival is unknown for patients who acquire extracorporeal cardiopulmonary resuscitation (ECPR). Furthermore, it is not known if treatment differs among centres, and if this difference and hospital case volume, are correlated with survival. There is centre level variability in post-resuscitation treatment for ECPR patients. This variability, and hospital annual case volume, are correlated with survival. An observational study of 4,296 adults was executed who received ECPR from the Extracorporeal Life Support Organization registry from 2014 until 2019. Tonna J, presented in a session at American Heart Association Scientific Sessions 2020: A Virtual Experience which analysed clinical variables within the first 24 hours following arrest, and hospital annual ECPR volume. The primary outcome was case-mix adjusted survival at hospital discharge, adjusting for factors previously correlated with survival following cardiac arrest or extracorporeal membrane oxygenation (ECMO). Mixed effects regression models were used to consider for clustering of outcomes by center. Case volume was layered into low (<6 cases/year), medium (6-12 cases/year) and high (>12 cases/year). Patient-level clinical variables following cardiac arrest, differed widely over individual hospitals, incorporating the use of percutaneous coronary intervention (PCI), mechanical venting of the left ventricle, and the use of inotropic medications. Increased ECMO circuit blood flow at 4 hours was correlated with survival (OR 1.14 per liter per minute of flow [95% CI 1.04 to 1.24]; p=0.004). Following 24 hours of ECMO, enhanced arterial pulsatility (OR 1.44 [95% CI 1.32 to 1.58]; p<0.001), the placement of a distal perfusion catheter (OR 1.79 [95% CI 1.19 to 2.67]; p=0.005), and the placement of a mechanical left ventricular vent (OR 1.37 [95% CI 1.07 to 1.76]; p=0.012) were all substantially correlated with survival. There was a no substantial correlation of the use of PCI following ECMO cannulation with survival (OR 1.31 [95% CI 0.998 to 1.91]; p=0.051). High case volume was not correlated with survival (OR 1.32 [95% CI 0.98 to 1.78]; p=0.072).
Clinical treatment of ECPR patients differs over hospitals. These clinical variables and treatments are correlated with survival; but centre volume is not.
Short- and Long-term Survival of Patients Supported on Venoarterial and Veno-venous Extracorporeal Membrane Oxygenation

The use of both venoarterial (VA) and veno-venous (VV) extracorporeal membrane oxygenation (ECMO) has been extended to include an expanded range of indications to assist patients in shock, but there is still minimal outcome evidence for these indications. Florea I, presented in a session at American Heart Association Scientific Sessions 2020: A Virtual Experience which analysed survival of VA and VV ECMO patients by indication. A systematic study of adults supported by ECMO was performed at a single cardiogenic shock center between January 2010 and November 2018. VA ECMO patients (n=449) and VV ECMO patients (n=91) were categorised as per indication for ECMO support. Kaplan-Meier analysis was used to form survival curves at 30 days and 1 year and log-rank test was used to compare them. Multiple comparisons were adjusted using post-hoc Tukey test. Acute Pulmonary Embolism (PE, n=14), Ischemic Cardiomyopathy or Myocardial Infarction (ICM or MI, n=108), Non-Ischemic Cardiomyopathy (NICM, n=82), Post-Cardiotomy (n=129), Transplant (Tx, n=32), and Other (n=84) were the subgroups of indication for VA-ECMO support. Kaplan-Meier estimates of survival were substantial; layered by indication at 30 days and 1 year (30d: p=0.006, 1y: p=0.009). Multiple comparisons were substantial for Acute PE v Post-Cardiotomy (30d: p=0.044, 1y: p=0.029), NICM v Post-Cardiotomy (30d: p=0.016, 1y: p=0.025), and Tx v Post-Cardiotomy (30d: p=0.01, 1y: p=0.022) at 30 days and 1 year. The subgroups of indication were ARDS: Influenza (n=25), ARDS: Other Infection (n=24), and ARDS: Non-Infectious (n=42) between VV-ECMO patients. No statistically substantial difference in survival was acknowledged among these indications either at 30 days (p=0.742) or 1 year (p=7.82).
Patients who need Post-Cardiotomy VA-ECMO support showed worse short- and long-term survival than patients who need support for Acute PE, NICM, or Transplant indications. However, no survival difference is acknowledged by indication between VV-ECMO patients.
Faster Time to Elevation of the Head and Thorax During Cardiopulmonary Resuscitation Increases the Likelihood of Return of Spontaneous Circulation After Out of Hospital Cardiac Arrest
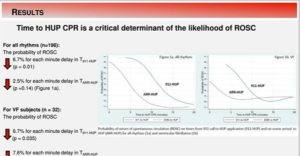
Device-assisted controlled sequential advancement increase of the head and thorax (HUP) with active compression decompression (ACD) or automated CPR with an impedance threshold device (ITD) improves consequences in animal cardiac arrest models. In the pre-hospital (EMS) setting, HUP CPR has recently started to be used. Moore JC, presented in a session at American Heart Association Scientific Sessions 2020: A Virtual Experience, which analysed the first use of a FDA approved HUP device on rates of spontaneous circulation (ROSC). From an IRB-approved HUP CPR registry of adult pre-hospital cardiac arrest patients, prospectively collected retrospective data was evaluated. Patients acquired HUP with 1) ACD + ITD CPR and/or 2) ITD+ automated CPR and/or 3) ITD + manual CPR. A restricted cubic spline analyses evaluated the probabilities of ROSC (ROSCprob) on times from 911 call to HUP application (T911-HUP) and on-scene arrival to HUP (TARR-HUP). Non-parametric descriptive statistics and tests of hypothesis were also utilized. 212 patients from 5 EMS sites from March 2019 to July 2020 were enrolled in the study and 198 patients completed the data. The ROSC rate was 30% (60/198), 62% (122/198) male with median age (IQR) 67 years (54-79). The median T911-HUP (minutes, IQR) among sites differed: 1) 6.4 (5.5-13.4) 2) 9.9 (6.6-10.6) 3) 15.9 (11.5-21) 4) 14.1 (10.7-18.2) 5) 19.0 (15.7-25.1), (p = 0.0001). The median TARR-HUP (minutes, IQR) also differed: 1) 2.7 (1 – 3.8) 2) 2.5 (1- 3) 3) 7.4 (3.3 – 13) 4) 6 (4 – 10) 5) 13.8 (9.1 – 18.8), (p =0.0001). In all patients, ROSCprob showed reduction by 6.7% for each minute delay in T911-HUP (p = 0.01), reduction by 2.5% for each minute delay in TARR-HUP (p =0.14) (Figure 1a). In patients with VF (n=32), ROSCprob reduced by 6.7% for each minute delay in T911-HUP (p = 0.035), and by 7.6% for each minute delay in TARR-HUP (p =0.028) (Figure 1b). 25/32 (78%) VF patients showed at least 1 failed shock earlier to HUP CPR.
Faster time to HUP CPR application is correlated with a greater likelihood of resuscitation. These findings must be contemplated while analysing and applying HUP CPR.
Tocilizumab Reduces Systemic Inflammation and Cardiac Injury After Out-of-Hospital Cardiac Arrest – Results from the Randomized Clinical Trial “Interleukin-6 Receptor Antibodies for Modulating the Systemic Inflammatory Response After Out-of-Hospital Cardiac Arrest (IMICA)”

Out-of-hospital cardiac arrest (OHCA) patients who remain comatose at admission are at great risk of morbidity because of the arising post cardiac arrest syndrome (PCAS). Systemic inflammation comprises a vital component of PCAS, and interleukin-6 (IL-6) is correlated with PCAS extremity. The IL-6 receptor antagonist tocilizumab could prospectively decrease inflammation in PCAS. Meyer MA, presented in a session at American Heart Association Scientific Sessions 2020: A Virtual Experience which analysed whether infusion of tocilizumab at admission decreases systemic inflammation following after OHCA of presumed cardiac cause and thereby prospectively mitigate organ injury. In a double-blinded placebo-controlled trial, 80 comatose OHCA patients were randomized (1:1) to a single infusion of tocilizumab or placebo, in addition to standard of care, incorporating targeted temperature management of 36°C for 24h. Blood samples were consecutively drawn in initial 72h. Primary endpoint: decrease in CRP. Secondary endpoints: markers of cardiac injury: CKMB, TNT, and NT-proBNP (only at 48h); brain: neuron-specific enolase (NSE). Continuous variables were log2 transformed and evaluated using mixed models to test for therapy-by-time interaction and time specific group differences; noticed values presented as mean [95%CL] following back-transformation.
There was a substantial impact of therapy across time in favor of tocilizumab for CRP, leucocytes, CKMB and NT-proBNP across the 72h period (all p<.01). Tocilizumab, active showed markedly reduction in CRP and leucocytes vs placebo at 48h, CRP 20 mg/L [15;27] vs 121 [104;140], and leucocytes 8 109/L [7;10] vs 12 [11;13], both p<0.01. Tocilizumab showed substantial reduction in CKMB, and TNT, with mean values peaking at 6 and 12 hours, CKMB: 6h active vs placebo, 40 ug/L [23;69] vs 66 [44;97], 12h 40 [23;70] vs 68 [46;100], both p<0.001; TNT: 6h 858 ng/L [498;1478] vs 1458 [1001;2124]; 12h 718 [404;1277] vs 1272 [848;1908]; both p<0.01. An active treatment showed substantial reduction in NT-proBNP at 48h (156 pmol/L [93;253] vs 254 [167;386], p<0.001). NSE levels did not vary among groups (p>0.2), nor survival at 180 days (64% vs 66%).
Tocilizumab therapy exhibited substantial decrease in systemic inflammation and cardiac injury in resuscitated comatose OHCA patients.
Association of Acute Exposure to Ambient Air Particulate Matter and Ozone with Risk of Out-of-hospital Cardiac Arrest
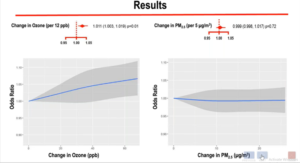
Malik A, presented findings of a study which assessed the association of acute exposure to ambient air particulate matter and ozone with risk of out-of-hospital cardiac arrest in a session at American Heart Association Scientific Sessions 2020: A Virtual Experience. The study investigated whether these ambient air pollutants are particularly associated with a higher risk of out-of-hospital cardiac arrest (OHCA). Under the Enhance Survival Cardiac Arrest Registry, 187,047 individuals were reported with non-traumatic OHCA that could be related to EPA data between 2013-2016. The exposure of a person to PM2.5 and ozone were estimated using data from the EPA’s Fused Air Quality Surface using a Downscaling tool, which combines monitoring station data with atmospheric models to forecast daily levels by census tract. By using a time-stratified case-crossover configuration, the links with acute exposure to PM2.5 and ozone with OHCA was examined. The day of the case was known as OHCA’s day. Associations were also measured over days 0-1 (lag 1) and days 0-2 (lag 2) for a moving average. Control days from the preceding 2 weeks were specified as the same weekday. Conditional logistic regression on PM2.5 and ozone was used to estimate associations, stratified by the patient. It was also investigated whether associations differed according to age, gender, ethnicity, and OHCA rhythm. Mean age was 62.6 ± 19.4 years, male 61.1% and non-White 52.6%. Mean concentrations of contaminants were 9.2 ± 4.9 μg/m3 PM2.5 on case day and 36.9 ± 12.1 parts per billion (ppb) ozone. With a 1.1% increase in OHCA odds per +12 ppb higher ozone level, a major ozone impact on the case day was observed. There was no correlation with PM2.5 on lag days or lag days, and no association with lag days with ozone. Age, sex, race and OHCA rhythm did not interfere with PM2.5 or ozone with OHCA-risk on either case or some lag days (p >0.2 for all).
Reverse exposure to higher levels of ozone in the U.S was observed, but not with PM2.5. It was associated with a higher OHCA risk. It is important to better identify the mechanisms by which acute ozone exposure increases the risk.
Collateral Damage: Hidden Impact of the Covid-19 Pandemic on Out-of-hospital Cardiac Arrest Event

Ball J, presented findings of a study, which assessed the hidden impact of the Covid-19 pandemic on out-of-hospital cardiac arrest event in a session at American Heart Association Scientific Sessions 2020: A Virtual Experience. During COVID-19, out-of-hospital cardiac arrest (OHCA) was identified by countries ravaged by huge case numbers and overwhelmed healthcare facilities. For countries where infection rates have been decreased, OHCA processes of care may also have been impacted by enforced limitations and treatment precautions. In Australia, personal protective devices, improvements in management to limit exposure, and the termination of a community co-responder network have disrupted time-sensitive OHCA initiatives. The effect of the limitations on the OHCA-of-care framework has yet to be explained. Almost 380 adults (age>15 years) with an attempted resuscitation between 16 March 2020 (State of Emergency declared) Compared with 12 may 2020 (Stage 3 restrictions lifted) with 1,218 cases occurring in 2017-2019 on the same dates, by using details from the Victorian Ambulance Cardiac Arrest Registry. During the pandemic period, initiation of resuscitation by paramedics declined dramatically (40.6% versus 46.9%, p=0.001). Patient age and gender distribution did not vary between the time ranges. In the pandemic era, arrests occurring in public areas decreased dramatically (10.0% versus 20.8%; p<0.001) and initial shocks of public access defibrillation/first responders also decreased (p=0.037). During the pandemic era, delays to key treatments increased, resulting in a median four-minute total delay during resuscitation attempts. As with patients presenting with ventricular fibrillation/ventricular tachycardia (VF/VT) (p=0.004), the proportion of OHCA patients discharged alive decreased by almost 50% (6.1% vs. 11.7%; p=0.002). A decrease in the number of survivors resulted in an estimated 35 excess deaths per million person-years, which if extrapolated over 12 months, corresponds to 186 excess deaths. Risk-adjusted discharge survival chances decreased by 54% during the pandemic phase (OR 0.46, CI 0.25-0.86 95%, p=0.015).
Although international studies have indicated reduced OHCA survival to COVID-19 infection rates, COVID-19 has been shown to cause collateral damage to the OHCA care system, resulting in considerably longer delays to key time-sensitive therapies. This did not however, fully justify survival declines.
Impact of the Covid-19 Pandemic on Survival Outcomes for Out-of-Hospital Cardiac Arrest
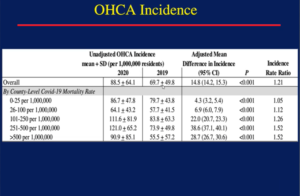
Chan PS, presented findings of a study, which assessed the impact of the covid-19 pandemic on survival outcomes in a session at American Heart Association Scientific Sessions 2020: A Virtual Experience. A substantial decrease in survival for out-of-hospital cardiac arrest (OHCA) has been found in recent studies from populations seriously impacted by the novel coronavirus 2019 (COVID-19) pandemic. Whether OHCA survival is pandemic-reduced in areas with a low to moderate burden of disease is uncertain. During the months of January to April 2019 and 2020, 52,186 OHCAs were registered in the cardiac arrest registry for enhance survival (CARES) in the U.S. The pre-pandemic (January-February), peri-pandemic (March 1-15), and pandemic (March 16-April) were graded as OHCAs in 2020. Cases were geocoded for U.S. counties, and COVID-19 mortality was classified as very medium (0-25), low (26-100), moderate (101-250), high (251-500) or very high (> 500) per 1,000,000 residents in each county during the pandemic time. In 2020 vs. 2019, Hierarchical Poisson regression models compared rates of sustained spontaneous circulation return (ROSC) and field resuscitation termination (TOR). After controlling for demographics and cardiac arrest variables (23.0% vs. 29.8%; adjusted RR 0.82 [95% CI: 0.78-0.87]), sustained return of spontaneous circulation (ROSC) rates were lower during the pandemic period in 2020 compared to 2019. In communities with high and extremely high COVID-19 mortality, respectively, sustained ROSC rates were 22% and 34% lower, but were also 11% and 15% lower in communities with very low and low COVID-19 mortality. After change, TOR rates were higher in 2020 (53.9% vs. 40.0%; adjusted RR, 1.27 [1.22-1.32]) and were higher in all populations, regardless of mortality from COVID-19. Compared to 2019, the incidence of OHCA in 2020 was largely greater in societies with a heavy burden of COVID-19. Importantly, sustained ROSC rates were comparable in 2020 relative to 2019 during the pre- and peri-pandemic eras.
Recent survival gains for OHCA in the U.S. were significantly undermined by the COVID-19 pandemic, including in populations with low COVID-19 mortality that did not experience a substantial rise in OHCA incidence.
In-Hospital Cardiac Arrest in Patients with Covid-19
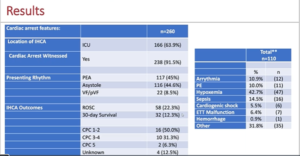
Mitchell OJ, presented findings of a study, which discussed about in-hospital cardiac arrest in patients with COVID-19 in a session at American Heart Association Scientific Sessions 2020: A Virtual Experience. In patients with COVID-19, the goal was to classify In-Hospital Cardiac Arrest (IHCA) outcomes and identify factors associated with good resuscitation and survival. Multicenter national retrospective cohort review of polymerase-chain-reaction (PCR) confirmed COVID-19 and IHCA adult patients. Using local quality improvement (QI) data bases and electronic medical records (EMR) billing codes, events were established. Using a Data Dictionary, data was manually extracted into the Research Electronic Data Capture (REDCap) database and analyzed using the χ2, Student t-test or Mann-Whitney U test, as needed. Via manual review of the EMR, the etiologies of IHCA and CPC scores were explored. From 03/01-05/31/20, a total of 137 IHCAs from 9 hospitals were included. The mean age was 65.6+15.0 years and 76.6% were male, respectively. Pulseless electric operation (62%), asystole (23%), and Ventricular fibrillation/ventricular tachycardia (VF/VT) (12%) were the initial rhythms. 71% required supplemental oxygen at the time of IHCA and 63% needed vasopressor/inotrope support. 40 % of ROSC was reached and 18% survived 30 days. 52% of 30-day survivors had 1 or 2 CPCs. When in the ICU, 74% suffered from IHCA: these patients were more likely to have sepsis (86% vs. 67%, p=0.031), hypotension (60% vs. 29%, p=0.001), and renal insufficiency in the 24 hours prior to their IHCA (45% vs. 26%, p=0.04). With 30-day survival varying from 2.6% to 100% and ROSC rates from 7.8% to 100 %, IHCA findings differed dramatically across hospital systems. Popular etiologies were hypoxemia (34%), sepsis (10%), arrhythmia (9 %), and pulmonary embolism (8%) when the IHCA cause could be established by the hospital arrest team.
The findings of a large COVID-19 IHCA cohort were presented and found that this population has better survival than previously suspected. Potentially reversible causes were prevalent. Both ROSC rates and discharge survival differed widely, indicating more study opportunities and improved performance.
Introduction of a Mechanical Chest Compression Device for In-hospital Cardiac Arrest during the Covid-19 Pandemic
Bhatnagar A, presented findings of a study, which discussed about mechanical chest compression device for in-hospital cardiac arrest during the Covid-19 Pandemic in a session at American Heart Association Scientific Sessions 2020: A Virtual Experience. For hospitalized patients during the COVID-19 pandemic, cardiopulmonary resuscitation (CPR) poses specific problems for resuscitation teams, including a possibly elevated risk of virus aerosolization. As such, advice has been released by the American Heart Association, which includes the proposed use if available, of mechanical chest compression devices. This research describes the experience of a high-load COVID-19 case tertiary care hospital, where mechanical compression devices were rapidly introduced early in the pandemic.
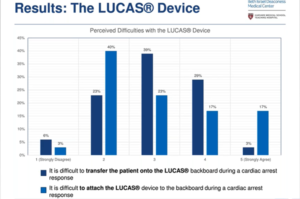
Two LUCAS® chest compression systems were deployed in April 2020 and workers were trained to use them. An electronic survey was established in June 2020, which analyzed the experiences of resuscitation providers who responded during the pandemic to in-hospital cardiac arrests (IHCA). The survey was sent to the leaders of the doctor code, anesthesiologists, and nurses in intensive care who responded to IHCAs. Of 76 surveys, 44 (58%) were returned. During the study period, there were 21 IHCAs. 15 (34%) of the respondents were nurses and 14 (31.8%) were medical trainees. In an IHCA where LUCAS® was deployed, 32 (73%) respondents were involved. 10 (31.3%) respondents agreed/strongly agreed that it was difficult to move to the LUCAS® backboard and that it was difficult to tie the LUCAS® to the backboard. 12 respondents (37.5%) claimed that LUCAS resulted in treatment in delays. 22 (68.8%) respondents thought that LUCAS® resulted in a more controlled resuscitation experience, 20 (62.5%) felt that LUCAS® increased the efficiency of chest compressions, and 23 (71.9%) indicated that less people in the room were allowed by LUCAS®. Patient size and difficulty attaching the device were identified as common obstacles by those who responded to arrests where the LUCAS® was not deployed.
Rapid implementation during the COVID-19 pandemic of mechanical chest compression devices is feasible. While there are major technological difficulties, a more regulated resuscitation experience, improved quality of compression and less people in the room are recorded by most. To achieve optimum outcomes, additional staff training may be required.
Risk of Covid-19 Illness among EMS Providers Following Cardiopulmonary Resuscitation and Aerosol Generating Procedures
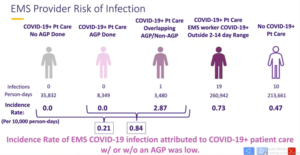
Brown AD, presented findings of a study which evaluated the risk of covid-19 illness among emergency medical services (EMS) providers following cardiopulmonary resuscitation and aerosol generating procedures in a session at American Heart Association Scientific Sessions 2020: A Virtual Experience. Providers of EMS can treat patients with COVID-19 without knowing the COVID-19 status of the patient. It is suspected that aerosol producing procedures (AGPs) increase occupational risk. The risk magnitude of AGPs is unknown when wearing personal protective equipment. The probability of EMS providers developing COVID-19 when AGPs were used vs. when not used during the treatment of patients with COVID-19 was compared. This retrospective cohort study classified patients with a positive COVID-19 nasopharyngeal swab (RT-PCR+) outcome from a nationwide COVID-19 registry within 10 days of an EMS experience in King County, Washington, between February 16 and July 31, 2020. AGPs have been identified as endotracheal intubation, supraglottic airway insertion, ventilation of the bag-valve mask, continuous positive airway pressure, oxygen non-rebreather mask (NRB), and drug therapy for nebulizer or metered dose inhaler. If the EMS provider’s RT-PCR+ test occurred about 14 days after the conference, COVID-19 transmission was attributed to the encounter. 1722 separate EMS providers who cared for 1155 COVID-19 patients were involved in 3231 EMS provider experiences. Of the 1383 COVID-19 patient encounters, 1176 involved no AGP and 207 had at least one AGP (Table). NRB oxygen (77%), positive pressure ventilation (28%), and advanced airways (19%) were the most common AGPs; chest compressions required 25 (12%). In all within 14 days of the COVID-19 patient experience, 3 of the 1722 specific EMS providers were RT-PCR+, 2 between AGPs and 1 without AGP. Overall, the incidence of EMS COVID-19 infection following occupational exposure was poor (0.93/1000 provider encounters), creating an unpredictable rate ratio that makes a substantial AGP contrast visible.
EMS COVID-19 occupational risk attributable to patient encounters was quite low. Interim case surveillance and continued analysis are ongoing to refine these results and enable robust comparison of AGP-specific risk.
