Priyadarsini R. IJSR. 2020 Mar;9(3):1-2.
Diabetic dyslipidemia is a complex cluster of potentially atherogenic lipid and lipoprotein abnormalities involving both quantitative and qualitative changes. Chronic hyperglycemia exerts a deleterious effect on the vascular wall and, by glycation of apolipoproteins, interferes with the normal pathways of lipoprotein metabolism. Increased plasma triglycerides, is linked to an active reductive synthesis pathway which involves increased G6PD activity being the major pathway for generation of NADPH. Glucose -6-phosphate dehydrogenase (G6PD) is the rate limiting enzyme of pentose phosphate pathway which produce NADPH the cells principal reductant involved in reductive biosynthesis of lipids. The current study was designed to correlate serum G6PD activity which produces NADPH and its association with dyslipidemia in Type 2 DM.
It is a Case Control hospital based study. Total 100 patients (76 males 24 females) with history of Type 2DM were selected from Medicine & Endocrinology OPD of MKCG Medical College. Equal age & sex matched healthy individuals were taken as controls. A morning sample of venous blood (5ml) was collected after overnight fast. The sample was analysed for G6PD, FPG, Fasting insulin and lipid profile. G6PD was measured by chemical method in semiauto analyzer. Estimation of cholesterol, triglyceride, HDL, VLDL and LDL was done in autoanalyzer. For serum lipid level, National Cholesterol Education Programme(NCEP) Adult Treatment Panel (ATP III) guidelines were referred. Statistical analysis was done by SPSS Version 20 software. In this study the mean age of diabetes mellitus patients is 52yrs as it is more common in middle age group. The anthropometric attributes like age, BMI, waist circumference, BP were elevated but not stastistically significant in diabetic patients when compared to healthy subjects (p>0.05). The levels of FPG level was found to be higher in diabetic cases which is stastistically significant. The mean of FI & HOMO-IR levels are higher in controls when compared with cases. The levels of TC, TG, LDL and VLDL were significantly higher in patient group as compared to controls, (p<0.05). The levels of HDL Cholesterol was found to be significantly lower in diabetics as compared to control group. Dyslipidemia is most frequently seen in diabetics and they are at greater risk of developing atherosclerotic diseases. Table 1 shows the Mean ± SD of G6PD the control and patient groups was 0.09 ± 0.06 and 1.92± 0.55 respectively. In our study the levels of G6PD was found to be higher in diabetic patients as compared to controls which is statistically significant. (Figure 1)
G6PD is positively and significantly correlated with Total Cholesterol (R2 = 0.680), Total Triglyceride (R2 = 0.358), LDL cholesterol (R2 = 0.549), VLDL Cholesterol (R2 = 0.385) but it is negatively correlated with HDL Cholesterol (R2 = -0.151 p= 0.033). (Table 2)
FBS is positively and significantly correlated with Fasting insulin (R2 = 0.483) and HOMA-IR (R2 = 0.676). On comparision it was observed that as the FBS level rises there is increase in Insulin Resistance (Table 3).
Thus, it was concluded that Increased activity of G6PD in diabetic cases, alters lipid homeostasis which leads to atherogenic abnormalities. Estimation of serum G6PD & its correlation with dyslipidemia can highlight its role in regulating lipid status in diabetes mellitus patients.
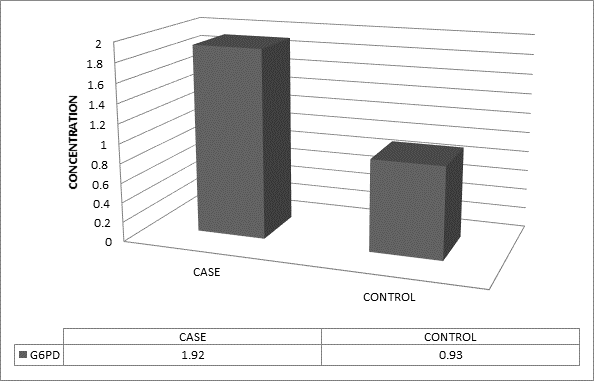
Figure 1: Mean of G6PD Activity in Cases and Control

Table 1: Comparison of Glucose-6-phosphate Dehydrogenase (G6PD) activity in diabetics and controls

Table 2: Correlation of Glucose –6- phosphate Dehydrogenase (G6PD) with Lipid Profile in diabetic patients

Table 3: – Correlation of Fasting blood sugar with Insulin Resistance in diabetic patients
