Coculescu B. J Enzyme Inhib Med Chem. 2019 Dec;34(1):783-788.
Heart failure is one of the real general medical issues where life expectancy might be prolonged by the capacity of the physician to build up an early diagnosis and to intercede to delay the term of the advancement of each pathophysiological phase of myocardial contractile deficit. Among the elements interceding in the development of cardiovascular pathology, not just at the endothelial coronary level, yet in addition at the degree of the myocardial syncytium, is likewise the osteopontin (OPN).
At myocardial level, OPN presents itself under two forms: stationary, situated in the interstitial matrix, and as a soluble cytokine, having the structure of the RGD field made up of the following amino acids: arginine–glycine–aspartate.
RGD intervenes the inter-activity with different integrins, incorporating that with 1-integrina overwhelmingly communicated in the myocardium. As illustrative of the transmembrane receptors, it gives through the solvent type of the OPN the communication between the extracellular matrix and the cardiomyocytes. These mentioned pathways permit the mediation of the matrix OPN whose amalgamation is invigorated by the angiotensin II (Ang II)– aldosterone system to intercede in the development of myocardial remodelling and fibrosis.
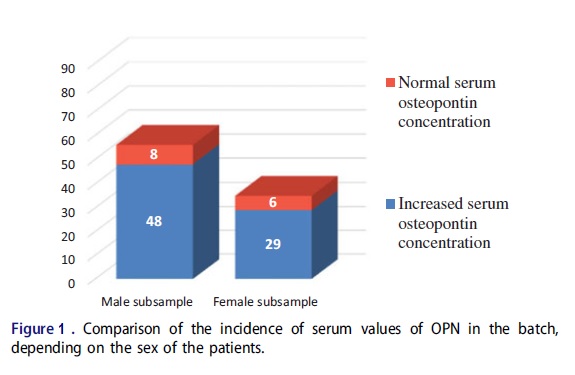
Coculescu et al., conducted a study to establish whether there are scientifically significant statistical arguments to support the admission of serum concentration of OPN as a biomarker of cardiac failure of ischaemic etiology and preserved systolic blood flow. 91 patients (35 women and 56 men) with chronic heart failure with myocardial ischaemia etiology were included in the study. On distribution of the cases as per normal and elevated serum values among each same-sex subgroup reported that physiological OPN serum concentration was present in only eight male and six female patients.
Figure 1 demonstrates that elevated serum OPN values are present in the batch at a rate of 78% (77 cases), 3.5 times higher than normal (14 cases = 22%). The incidence of increases might be considered as around indistinguishable among both the male and the female subsample, despite the fact that there is a marginally distinction of 2.5% for the male gender.
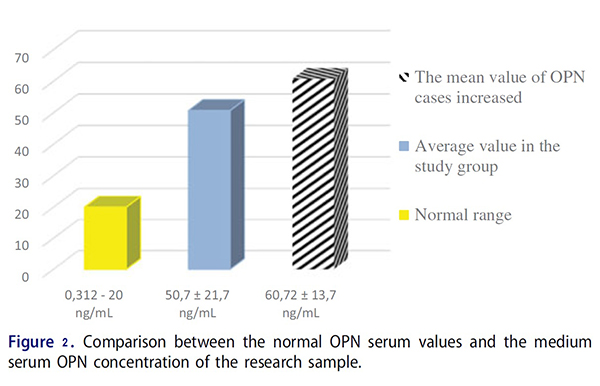
The comparison between the mean serum concentration and standard deviation values of OPN in patients with diastolic dysfunction with those of circulating OPN levels normally admitted in healthy subjects reveals a net increase, even if the ejection fraction is not affected (Figure 1). In this manner, the increase in mean serum OPN is 2.5 times higher than the upper limit of normal circulating.
The medium serum OPN concentration was calculated for the entire sample based on the individual results for the biomarker, also including the patients with normal values, as presented in the following figure 2.
For the patients studied, in the case of patients with normal serum values of OPN, the results were:
Male cases with normal serum OPN values = 8 cases = 4:5% _______________________________________ ___________ ________
Female cases with normal serum OPN values 6 cases 17%
Thus it could be concluded that there is occurrence of elevated OPN serum in men, 1.7 times compared to that in women, permits to concede and guarantee that the processes of myocardial reshuffle (hypertrophy and fibrosis) among the patients with DHF by IHD are more frequent and more intense in men than women.
