Chopra HK, et al. Circ Res. 2019 Mar 29;124(7):984-986.
The leading cause of global cardiovascular mortality and morbidity is systemic hypertension. This is a condition which can be easily diagnosed and without much costs. Uncontrolled hypertension causes target organ damage and substantial disorder burden on the community. Hence, it is obligatory to preserve and protect public health in India with aggressive control of hypertension. Nearly 18 million deaths annually were caused by cardiovascular disease (CVD). 30% of global deaths were owned to CVD regardless of the phenomenal development in disease management. The American guidelines and the European guidelines suggested the same therapeutic BP goal of <130/80 mm Hg. (Figure 1A) The occurrence of hypertension is nearly 60% in the elderly (>70 years) in India. India is under a long stretch of escalating incidence of hypertension arbitrated disorder which is pummelling and demolishing the health of its citizens. (Figure 1B)

Figure 1. A, Latest hypertension guidelines 2017/2018. B, Financial burden from CVD-INDIA. CVD indicates cardiovascular disease; and HTN, hypertension.
There is vast occurrence in the Indian population showing that BP levels among 130 to 139/80 to 89 mmHg cause significant CVD, stroke, and premature mortality. (Figure 2)
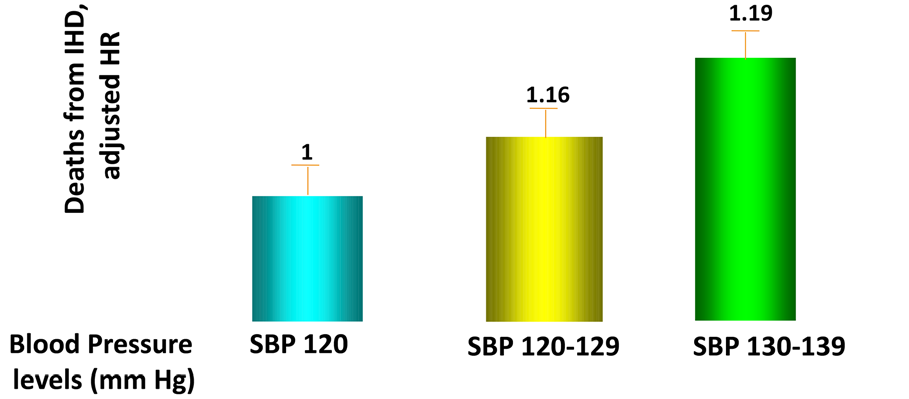
Figure 2: Deaths from ischemic heart disease and blood pressure levels from Mumbai/India cohort study. SBP indicates systolic blood pressure.
The European hypertension guidelines have recognized South Asians as the highest risk category and most exposed to the outcomes of increased BP. Additionally, high uric acid level is an added risk factor in patients with hypertension; hyperuricemia is common in Indian patients with hypertension. There is sufficient corroboration that BP levels among 130 to 139/80 to 89 mmHg causes significant CVD complications and therefore, a goal BP of <130/80 mmHg should be recommended for most patients with hypertension. Hypertension awareness is low because of urban-rural differences in health care approach and disruption of disease prevention pathways in the country. Any broad national policy for the non-communicable disease (NCD) has to permeate to the grassroots. More than 54% of total deaths in India happened due to NCDs, out of which CVDs provided a share of 25%. A multidimensional inclusive preventive measure has to be taken as the country has been witnessing a steady increase in BP levels, cholesterol levels, glucose levels, body weight, sedentary life-styles, and unhealthy nutrition over decades. A coronary heart disease at younger age (<40 years) is developed in Indians irrespective of their geographic or expatriate status. Massive screening check-ups should be done for hypertension however with a guaranteed follow-up and analysis. BP measurements should be accessible at public places like airports, railway stations, shopping malls, hospital lobbies, bank lobbies, and at the workplace to develop awareness about hypertension and its consequences. The prevalence of hypertension in India has to be decreased by 25% and secondary prevention by 50% to meet the aim of reducing the CVD mortality by 25% by 2025. India has majorly retrieved in communicable diseases; it can repeat the same logic and magic in restraining NCDs as well!
Thus, it was concluded that the Indian hypertension guidelines should be amended to recommend more aggressive BP reduction as instructed by the current unfavourable trends in CVD because of uncontrolled hypertension.
