Nguyen Q, et al. Front Cardiovasc Med. 2019 Oct 22; 6:151.
Nguyen Q, et al., conducted a study to determine the adequacy of the Kansas City Cardiomyopathy Questionnaire (KCCQ-12) to conclude Supportive Care (SC) requirement in an ambulatory HF patient population and secondly, interpret the effect of a multidisciplinary model of SC integrated into a contemporary HF clinic.
Approximately 456 patients allocated to take part in the study and fully completed the KCCQ-12. During study recruitment visit, HF patient filled out the KCCQ-12. Along with a study team member, through interview, patient details and medical history were assembled. Other consistent details which include medications, hospitalizations for HF, and any related outcome events (stroke, myocardial infarction, kidney, or liver failure) were also documented. As a screening tool, the shortened version KCCQ-12 were used for SC need in ambulatory HF patient population using a KCCQ-12 summary score of <29 as the cut-off.
Symptom frequency, physical and social limitations, and quality of life impairment as a result of HF were estimated in Figure 1. Due to HF, jogging or hurrying was affected in approximately 40% of patients signifying that they were “extremely limited” in the activity (Figure 1). By using the cut-off KCCQ-12 summary score of <29, out of 456 patients, 41 (9%) had SC needs (Figure 2A). The median scores for each of the 4 domains for patients with and without SC needs were measured (Figure 2B). Twenty-three patients were referred to the newly established SC clinic (SCC) (Figure 3A). Almost 23 patients were referred to SC clinic, out of 23 patients, 2 died before being seen, 20 received SCC and 1 refused SC. Among 20 patients who received SCC, 11 died and 9 are currently being followed (Figure 3B). Almost 17 patients had available KCCQ-12 summary scores in the original SC cohort of 23. Nevertheless, out of 17 (35%), only 6 had KCCQ-12 scores <29 which indicates the need for additional assessment tools in this patient population.
Thus, the importance of unmet supportive care needs in HF patients is significant. Whereas, the KCCQ-12 questionnaire is a beneficial tool to recognize patients with SC, sequential clinical evaluation, establishment of a SC clinic and prompt referral are essential for patients needing supportive care.
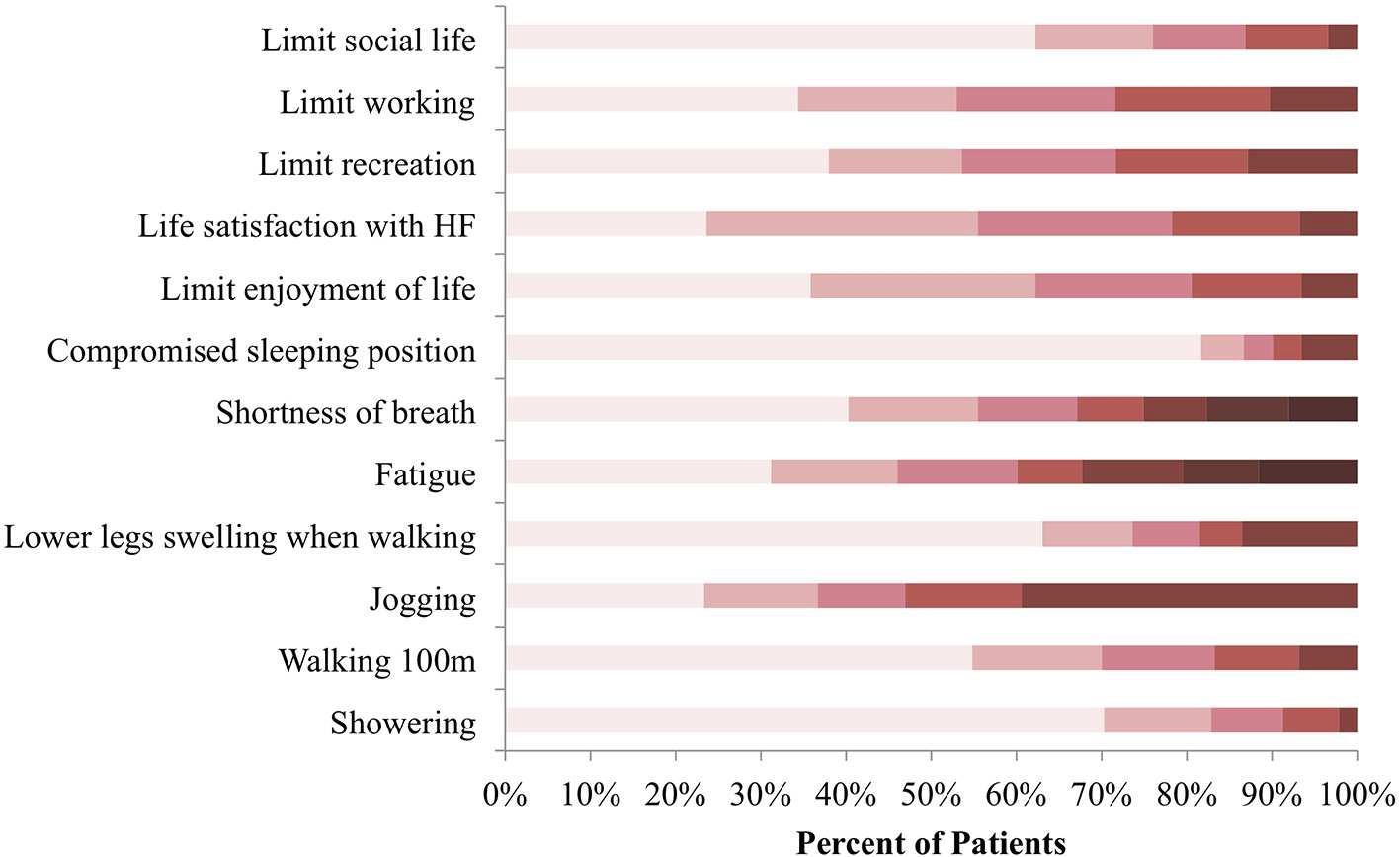
Figure 1: KCCQ-12 response distribution at baseline. Symptom burden, physical and social limitations, as well as quality of life impairment was reported in reference to the preceding 2 weeks before consultation. Colors categorize responses in terms of how limited patients were in the listed activities, with darker shades representing extreme limitation and lighter shades representing minimal to no limitation N = 456.
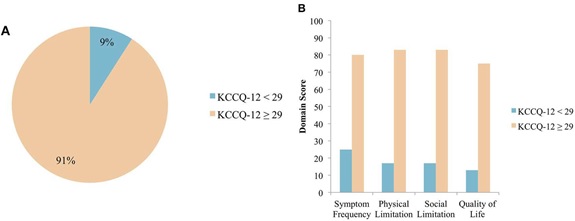
Figure 2: (A) Distribution of patients with HF requiring SC, grouped by KCCQ-12 summary score. Using a KCCQ-12 summary score cut-off of <29, 9% of patients with HF require SC N = 456. (B) Median domain scores in patients with and without SC needs. Median scores across the 4 domains as assessed by the KCCQ-12 are shown, with patients grouped according to the chosen KCCQ-12 cut-off score of <29 N = 456.
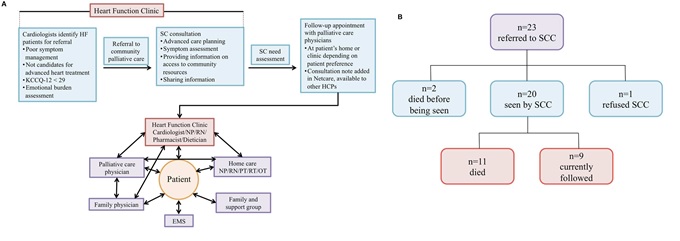
Figure 3: A) Supportive care model for patients with HF. Schematic model of SC integrated into routine care for patients with HF at the Heart Function Clinic. HF, heart failure; SC, supportive care; HCPs, health care providers; NP, nurse practitioner; RN, registered nurse; PT, physical therapist; RT, respiratory therapist; OT, occupational therapist; EMS, emergency medical services. (B) Overview of heart failure patients referred to SCC. Twenty-three patients were initially referred to SC clinic (SCC).
