
Population Screening Reveals Early-Stage Type 1 Diabetes in Children and Predicts Progression to Clinical Disease
A large population-based screening study published in JAMA examined more than 220,000 children in Germany to detect early, presymptomatic type 1 diabetes using islet autoantibody testing. The study aimed to understand how common early-stage disease is and how it progresses over time in the general pediatric population.
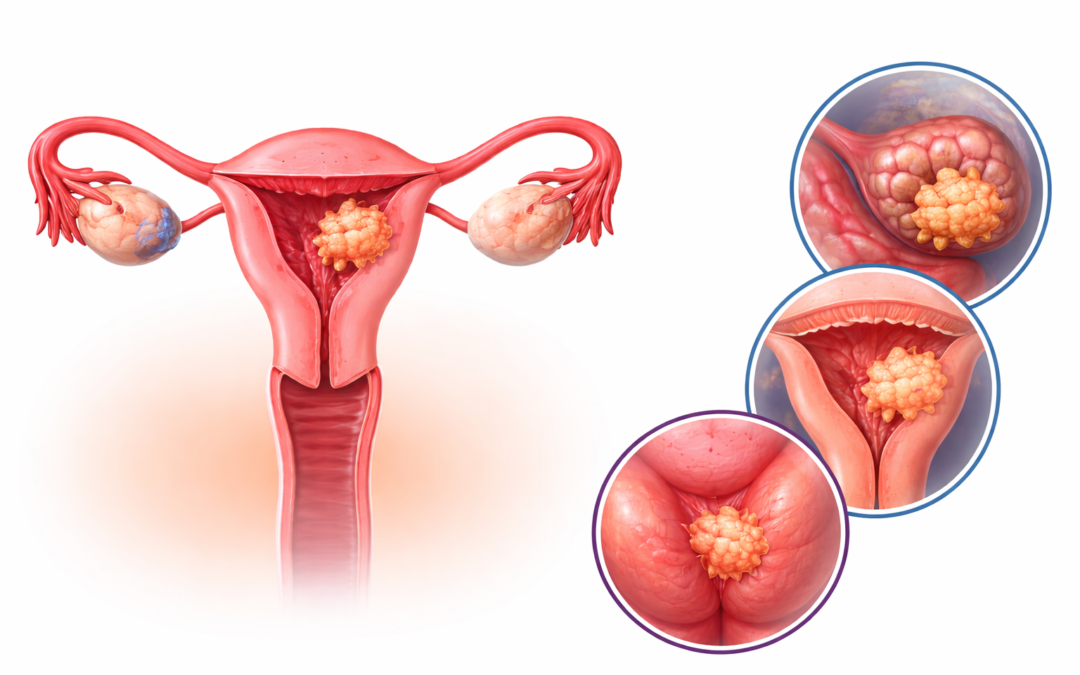
GSK Showcases Promising B7-H4 ADC Data in Gynaecological Cancers
GSK has reported promising clinical data for its investigational B7-H4-targeted antibody–drug conjugate (ADC), mocertatug rezetecan (also known as GSK5733584), in patients with gynaecological cancers, including ovarian and endometrial malignancies. These cancers often present at advanced stages and are associated with poor prognosis, particularly in patients who develop resistance to standard therapies such as platinum-based chemotherapy. The emergence of targeted therapies like ADCs represents a significant advancement in addressing these unmet clinical needs.

Oral Wegovy Outperforms Orforglipron in Weight Loss and Tolerability
The emergence of oral glucagon-like peptide-1 (GLP-1) receptor agonists marks a significant advancement in obesity pharmacotherapy, offering needle-free alternatives to injectable agents. In this context, a new population-adjusted indirect treatment comparison (ITC), to be presented at the Obesity Medicine Association (OMA) 2026 annual meeting, evaluated the relative efficacy and tolerability of oral semaglutide 25 mg (Wegovy® pill) versus orforglipron 36 mg.

Prof GIUSEPPE MANCIA

Prof. Enrico Agabiti Rosei at ESH 2019 Milan part 1
Prof. Enrico Agabiti Rosei at ESH 2019 Milan part 2

Professor Dame Anna Dominiczak at ESH 2019 Milan
