Cerebral Oximetry During Pediatric In-hospital Cardiac Arrest

Regional oxygen saturation (rSO2) estimated by cerebral near-infrared spectroscopy (NIRS) during cardiopulmonary resuscitation (CPR) is correlated with spontaneous circulation (ROSC) return and hospital discharge (SHD) survival in adults with minimal data in children. Esangbedo ID, presented a study in a session at American Heart Association Scientific Sessions 2020: A Virtual Experience, which hypothesized mean cerebral rSO2 in pediatric in-hospital cardiac arrest (IHCA) would be correlated with return of spontaneous circulation (ROSC). 3 sites outlined the consecutive case series of pediatric IHCA occurrences with rSO2 data during 2016-2020 to the Pediatric Resuscitation Quality (pediRES-Q) collaborative. Patients with CPR duration ≤2 minutes or who had return of circulation via extracorporeal membrane oxygenation were excluded. A mean rSO2 for duration of CPR was measured and the primary outcome estimate was ROSC. Exploratory sensitivity analyses were executed for cutoffs of mean rSO2 >25, >30, >35, >40 and >50%. An independent samples t test, exact logistic regression and Fisher’s exact test was used for analysis.
From the 36 occurrences (26 index), median age was 3 [IQR 1,7.8] months; 29 (80.5%) showed congenital heart disease and 15 (41.7%) showed single ventricle (SV) physiology. Median CPR duration was 7.5 [IQR 3.8, 32.2] minutes and 28/36 (77.8%) exhibited ROSC. ROSC group exhibited 44.2% (±19.5) of mean intra-arrest cerebral rSO2 vs. 37.4% (±15) for non-ROSC group (p=0.267). No correlation was found among rSO2 and ROSC, even after controlling for age, presence of congenital heart disease, and SV pxact logistic regression. No substantial correlation was found with ROSC using mean rSO2 cutoffs >25, >30, >35, >40, and >50%. The SV subgroup showed same result.
No substantial correlation was found among cerebral rSO2 during pediatric cardiac arrest and ROSC in this small pediatric cohort of predominantly cardiac patients, even after controlling for significant confounders of age and SV physiology. More extensive studies with larger populations, and analysing intra-arrest change in cerebral rSO2 from baseline, are affirmed to yield more insights into the possibilities of using rSO2 to lead CPR.
Non-invasive Measurement of Cerebral Tissue Oxygen Extraction Fraction is Correlated with Microdialysis Brain Injury Biomarkers During Extracorporeal Cardiopulmonary Resuscitation
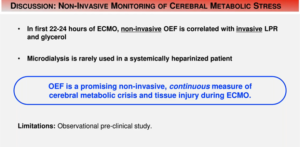
After prolonged or unsuccessful resuscitative efforts, extracorporeal membrane oxygenation (ECMO) assisted CPR (ECPR) can enhance consequences, however neurological injury remains frequent in survivors. The absence of routine neuromonitoring in ECPR and ECMO constrains brain-targeted management to aid enhanced neurological outcomes. Ko TS, presented a study in a session at American Heart Association Scientific Sessions 2020: A Virtual Experience, which analysed the correlation of non-invasive, frequency-domain diffuse optical spectroscopy (FD-DOS) measurements of cerebral tissue oxygen extraction fraction (OEF), an indicator of metabolic stress, with invasively gathered brain injury biomarkers to investigate the utility of this monitoring modality in ECPR. FD-DOS measurement of cerebral OEF is positively associated with biomarkers of brain injury (lactate-pyruvate ratio, LPR; glycerol).
FD-DOS continuously monitored cerebral OEF in 9 pediatric swine (8-11 kg) who underwent 30-60 minutes of manual CPR, were cannulated for ECMO, and endured on ECMO for 22-24 hours. Cerebral pyruvate, lactate, glycerol and glucose content were estimated from cerebral microdialysate samples gathered hourly. The association among OEF and microdialysis parameters were evaluated by a linear mixed-effects model including subject-specific random slope and intercept effects. Consequence was ascertained at p<0.05. Microdialysis parameters were compared to non-invasive OEF values from 192 samples. OEF was substantially associated with LPR (p=0.001), and relative change in glycerol (p=0.005) and glucose (p=0.020) concentrations from baseline.
Non-invasive FD-DOS neuromonitoring of OEF showed substantial assciations with invasive brain injury biomarkers; elevating OEF was correlated with increased LPR and glycerol, and decreased glucose. FD-DOS perception of critical neurometabolic stress at the bedside may facilitate brain-targeted ECMO treatment following cardiac arrest.
Hyperoxemia is Associated with Poor Neurological Outcomes in Patients with Out-of-hospital Cardiac Arrest Rescued by Extracorporeal Cardiopulmonary Resuscitation: Insight from the Nationwide Multicenter Observational JAAM-OHCA (Japan Association for Acute Medicine) Registry

Previous studies have shown a correlation among hyperoxemia and mortality following cardiopulmonary resuscitation (CPR) in out-of-hospital cardiac arrest (OHCA) patients; but, there is a lack of evidence for patients undergoing extracorporeal CPR (ECPR). Nishihara M, presented a study in a session at American Heart Association Scientific Sessions 2020: A Virtual Experience, which assessed the hypothesis that hyperoxemia is correlated with poor neurological outcome in patients managed by ECPR. The Japanese Association for Acute Medicine – OHCA (JAAM-OHCA) Registry is a multicenter, prospective, observational registry incorporating 34,754 OHCA patients during 2014 and 2017. Patients who had been revived and survived 24 hours following OHCA and showed a PaO2 levels above 60 mmHg were incorporated. Eligible patients were distributed into 2 groups by each 2 definition as per the PaO2 levels estimated from arterial blood gas evaluation 24-h after the ECPR, (1) High-level of PaO2 (H-PaO2, n=242) as PaO2 ≥ 157 mmHg (median) and control (n=211) as 60 < PaO2 < 157 mmHg, (2) hyperoxemia (HO, n=80) as PaO2 ≥ 300 mmHg and control (n=373) as 60 < PaO2 < 300 mmHg. The primary and secondary outcomes included the favorable neurological outcome, described as Cerebral Performance Categories (CPC) Scale 1-2, and survival at 30 days after OHCA, respectively.
453 patients with ECPR were incorporated from the 34,754 patients with OHCA. H-PaO2 and HO group showed substantially lower number of CPC 1-2 as compared to each control group (H-PaO2: 17.4% vs. 33.2%; OR 0.42; 95% CI 0.27-0.66; p<0.0001, HO: 8.8% vs. 28.2%; OR 0.24; 95% CI 0.11-0.55; p<0.001). The high oxygen groups showed lower 30-day survival (H-PaO2: 39.3% vs. 57.4%; OR 0.48; 95% CI 0.33-0.70; p<0.0001, HO: 25.0% vs. 52.6%; OR 0.30; 95% CI 0.17-0.52; p<0.0001). The H-PaO2 and HO were correlated with unfavorable neurological outcomes after adjusting for potential confounders (adjusted OR, H-PaO2; 2.71; 95% CI 1.16-6.30; p=0.021, HO; 5.76; 95% CI 1.30-25.4; p=0.021). The H-PaO2 and HO were also correlated with poor 30-day survival (adjusted OR, H-PaO2; 2.28; 95% CI 1.13-4.60; p=0.021, HO; 3.75; 95% CI 1.28-11.0; p=0.016).
In OHCA patients with ECPR, hyperoxemia was correlated with worse neurological consequences.
Identification of Decreased Plasma Lysophosphatidylcholine Using Phospholipidomics in Cardiac Arrest: A Novel Therapeutic Application
Cardiac arrest (CA) is an important public health burden with few efficacious treatments available. Plasma phospholipids are significant for proper organ function. It was hypothesized that modifications in plasma phospholipids may play a significant role in the pathophysiology of CA and normalizing these modifications may be a unique therapeutic application for the management of CA. Nishikimi M, presented a study in a session at American Heart Association Scientific Sessions 2020: A Virtual Experience, which examined the phospholipid treatment as an unique therapeutic approach in CA.
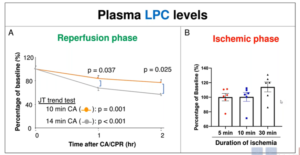
The plasma samples were collected from CA patients and controls from North Shore University Hospital. Phospholipidomics was performed on them to recognise plasma phospholipids that associate with injury extremity. The finding was confirmed using rat model of 10 and 14 min of asphyxia-induced CA. Eventually, the impact of administering LPC was analysed using the same model. From the phospholipids evaluated, CA patients had substantial reduction in the lysophosphatidylcholine (LPC) levels, which was also correlated with survival of patients. The same trend was noticed in the rat model where rats after 14 min CA showed substantially lower plasma LPC levels as compared to rats after 10 min CA. LPC levels also began to reduce continuously after resuscitation, however not between the ischemic phase of CA. In the end, it was found that LPC administration significantly elevated rat survival than control group. Rats who survived in the LPC-treated group showed substantially enhanced brain function and improved brain histology supporting supported the neuroprotective effect of LPC. LPC therapy enhanced plasma IL-10 levels and reduced IL-6 levels post-CA.
Plasma LPC levels inversely associated with survival and LPC therapy showed substantial enhancement in brain function and rat survival. This data states that the reduction of plasma LPC is a vital procedure responsible for brain damage exhibiting the prospective of LPC as a unique therapeutic in CA.
Capnographic Differences in Out-of-hospital Overdose-related, Respiratory, and Cardiac Arrests
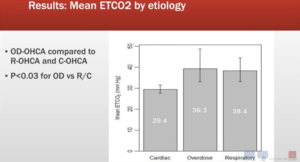
The ventilatory dimensions of overdose-related OHCA (OD-OHCA) are little understood. Spaite DW, presented a study in a session at American Heart Association Scientific Sessions 2020: A Virtual Experience, which compared maximum ETCO2 (mETCO2; each patient’s highest CO2 level) and mean for each recorded minute of CPR in OD-OHCA to that of respiratory (R-OHCA) and cardiac (C-OHCA) arrests.
Continuous CO2 data (Zoll E/X series monitors) were collected from 3 Arizona EMS agencies. Cases showed at least 3 min of recorded CO2 in CPR. Arrests were categorised as OD-OHCA by EMS and/or hospital documentation. Any drug OD was incorporated (e.g., opioids, mixed). C-OHCA and R-OHCA cases were randomly selected for comparison. Fisher’s exact test was used to compared the groups or Chi-squared for categorical and Kruskal-Wallis for continuous variables.
263 patients were enrolled (37 OD-OHCA, 157 C-OHCA and 69 R-OHCA; median age 61, 64% male, 1/10-12/18) with 10,271 min of data [median resuscitation interval 37 min (IQR 29, 47)]. Mean ETCO2 (SD): OD-OHCA [41 mmHg (24)]; R-OHCA [40 (23)], C-OHCA [30 (13); p<0.01]. Median mETCO2: OD-OHCA [57 mmHg (95CI: 50, 77)]; R-OHCA [61 (50, 73)], C-OHCA [48 (44, 50); p<0.001;]. While mean ETCO2 and mETCO2 were similar for OD-OHCA and R-OHCA, they were both substantially greater as compared to C-OHCA (p<0.01 for all comparisons). In OD-OHCA, ETCO2 waveforms mirrored the very high, full waveforms typical of R-OHCA although those in C-OHCA likely to be low and blunted.
This is the first report of continuous capnography in resuscitation of OD-OHCA. The mean ETCO2 and median of mETCO2 of OD-OHCA and R-OHCA indicate similar physiology (hypoventilation and hypercapnia leading to arrest). Both etiologies showed much greater ETCO2 values than C-OHCA, where low blood flow brings minimal CO2 to the lungs and provides low, and morphologically different, waveforms. Future studies are required for evaluating OD arrest physiology and various approaches to resuscitation and pharmacological reversal.
Multicenter Evaluation of Etiology and Observed Transition Intensities Between Pulseless Electrical Activity and Return of Spontaneous Circulation
Cardiac arrest presents with one of three clinical conditions; Cardiac standstill (asystole), Pulseless Electrical Activity (PEA), or ventricular fibrillation/tachycardia (VF/VT). Multiple etiologies lead to PEA and account for most in-hospital cardiac arrests. Unneland E, presented a study in a session at American Heart Association Scientific Sessions 2020: A Virtual Experience, which assessed the dynamic nature of transitions in and out of PEA, in terms of hospital sites and presumed etiology.
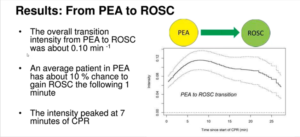
538 episodes of cardiac arrest were evaluated at one Norwegian hospital and 3 U.S. hospitals. ECG, chest compressions and ventilations were recorded by defibrillators in CPR. Each event was evaluated by a graphical application. The transition intensity was estimated, i.e. the immediate probability of a transition given the current condition, among PEA and ROSC by Aalen’s additive model for time-to-event data. 0.10 min -1 was the overall transition intensity from PEA to ROSC, so about 10 % chance was there to obtain ROSC the following 1 minute to an average patient in PEA. The intensity culminated at 7 minutes of CPR, with some heterogeneity among hospitals (0.07 to 0.11 min-1). The reverse transition intensity was rather constant at 0.10 min -1 (range 0.05-0.11) from ROSC to PEA. Information concerning assumed cardiac or non-cardiac etiology was accessible in 208 episodes (123 cardiac). Patients with a cardiac etiology showed a marginally smaller (-0.03 min-1) from PEA to ROSC, chance of making the transition (p=0.049), however etiology did not effect on the ROSC to PEA transition (p=0.39).
An overall intensity of 0.1 min-1 was noticed for transitions among PEA and ROSC, with some hospital heterogeneity. This may be because of heterogeneity in the underlying patient populations. The chances of transitioning from PEA to ROSC was found to increase from the start event recording until an average peak intensity at 7 minutes. This data may enhance the clinicians’ understanding of the procedure from PEA to ROSC.
Machine Learning-based Dispatch Rule for Drone-delivered Defibrillators
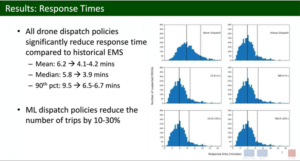
Leung KHB, presented a study at American Heart Association Scientific Sessions 2020: A Virtual Experience, which reported the all suspected Out of Hospital Cardiac Arrest Care (OHCA) in Peel Region, Ontario, Canada from January 2014 to December 2019. Neural Network Model for Predicting Emergency Medical Services (EMS) Response Time Using OHCA Location, Response Ambulance Distance, Day of Week and Day Time Qualified. Instead of the least square loss, the model optimized loss function that penalized the weighted errors in the dispatch decision (type I/II error). Assuming drones were deployed from three bases in the area, drone response time for each suspected OHCA was calculated using actual drone specifications. The dispatch rule dispatched a drone when its measured response time was shorter than the planned EMS response time. Response time was determined as the minimum response time for drones and EMS. The performance of the dispatch rule was compared with out-of-sample OHCAs using 5-fold cross-validation in the baseline cases of (1) no drones and (2) drone dispatch to any suspected OHCA. Statistical analysis of the median response times was conducted using a right-size sign test. 4774 suspected OHCAs with a median historical response time of 6.0 minutes to the EMS were reported. The median answer time was slightly shorter at 3.9 minutes (p<0.001) using the dispatch rule. Drones were sent to 3803 cases (79.7%) and the drone response was faster than EMS in 3076 cases (80.9%). If the drone was not dispatched, it would have been slower than the EMS in 856 cases (88.1%). Sending a drone to any suspicious OHCA resulted in a similar median response time of 3.9 minutes (p<0.001), with drones arriving before EMS in 3191 cases (66.8%).
Similar response times are accomplished by a machine-based dispatch rule as a policy that dispatches a drone to all suspicious OHCAs, while dispatching drones less frequently.
Annual and Lifetime Economic Productivity Loss Due to Adult Out-of-hospital Cardiac Arrest in the United States
Coute RA, presented a study at American Heart Association Scientific Sessions 2020: A Virtual Experience, which assessed the annual and lifetime economic productivity loss due to adult out-of-hospital cardiac arrest (OHCA) in the United States (U.S.).
All adult (age ≥ 18 years of age) non-traumatic EMS-treated OHCA with complete age, sex, race and survival data from the CARES database for the most recently available 5-year period were included. Annual and lifetime labor productivity values, based on age and gender, were extracted from previously published national economic data. Productivity losses for OHCA activities were measured on a yearly basis. Survivor productivity losses were allocated to the cerebral output category (CPC) score: CPC 1 and 2 = 0 % productivity loss; CPC 3-5 = 100 % productivity loss. Sensitivity analyzes were carried out to attribute CPC 2 to varying productivity losses (0-100%). Lifetime productivity values assumed a 1% annual growth rate and a 3% discount rate. Productivity statistics was provided in U.S. dollars and adjusted for inflation in 2016 values. Results for the annual U.S. population were extrapolated. Inclusion requirements were met in a total of 338,492 (96.5 %) cases. In 2018, the total annual and lifetime productivity losses per OHCA were $ 48,224 and $ 638,947. Total annual and lifetime production losses were $3.8 billion and $50.6 billion for the sample population in 2018, respectively. Sensitivity analyses that attributed varying productivity losses to CPC 2 reported similar results. Compared to females, males had a much greater loss of productivity lifetime to around 65years of age. The estimated annual and lifetime production losses due to OHCA were $ 11.3 billion and $ 150.2 billion, respectively, for the U.S. population in 2018.
Significant annual and lifetime economic production losses are associated with adult non-traumatic OHCA incidents and should be the priority of public health services to enhance prevention strategies and survival outcomes.
Association of Epinephrine Prior to Defibrillation with Survival in Patients with In-hospital Cardiac Arrest
Evans E, presented a study at American Heart Association Scientific Sessions 2020: A Virtual Experience, which assessed adults (>18 years) who have been diagnosed with an index In-hospital Cardiac Arrest (IHCA) due to an initial shockable rhythm, using the 2000-2018 get the resuscitation data guidelines. A time-dependent propensity-matched study was performed to assess the relationship of epinephrine with discharge survival and acute resuscitation survival prior to first defibrillation (i.e., restoration to spontaneous circulation for >20 minutes).
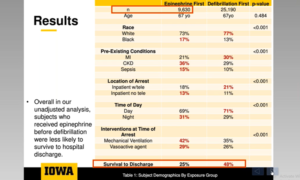
10,057 (29.0%) obtained epinephrine prior to defibrillation among 34,688 topics. In both classes, the median age was 67 years. Patients in the first category of epinephrine were less likely to have myocardial infarction or heart failure compared to defibrillation first, but more likely to have renal failure, sepsis and pneumonia, to be placed in the intensive care unit, and to be ventilated mechanically (p< 0.001 for all). Epinephrine therapy was initially closely correlated with a delay in first defibrillation (median 3 min vs. 0 min; p<0.001). Epinephrine prior to defibrillation was associated with lower chances of discharge survival (OR: 0.81, 95% CI0.76 – 0.86) and acute resuscitation survival (OR: 0.79, 95% CI 0.74 – 0.84) in the propensity-matched study. Lower survival (OR: 0.87, 95% CI 0.78-0.97) and acute resuscitation survival (OR for acute resuscitation survival: 0.83,95% CI 0.74-0.93) were correlated with early epinephrine, also in patients who received defibrillation within 2 minutes.
Despite a heavy focus on prompt defibrillation in current guidelines, epinephrine was received before first defibrillation by almost 1 in 3 IHCA patients due to a surprising rhythm. Epinephrine was related to worse survival outcomes prior to defibrillation. Although defibrillation delays were more frequent in the early epinephrine community, even in patients who received prompt defibrillation, early epinephrine remained associated with worse outcomes.
Barriers and Opportunities for a Drone-Delivered AED Network in Durham, North Carolina
Starks MA, presented a study at American Heart Association Scientific Sessions 2020: A Virtual Experience which examined barriers and opportunities for a drone-delivered AED network in Durham, North Carolina. The goal was to define stakeholder attitudes towards drone-based emergency care production for out-of-hospital cardiac arrest.
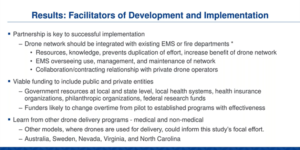
Using qualitative methods, key stakeholder perceptions about the use of a drone to deliver automated external defibrillators (AED), barriers and facilitators, implementation considerations, and long-term sustainability factors for the early establishment of a drone AED network were analyze. Based on professional status, 22 key individuals listed as potential respondents; 16 respondents participated in data collection. Participants in the research included government, health, emergency services, industry, culture, and aviation (regulation and drone operation) leaders. Interview data was collected and transcribed; NVivo was used to analyze data. Based on constructs found in previous literature and inductive consideration of the data from this study, including both thematic and descriptive coding, a coding scheme was developed. Wide support has been established for a drone-delivered AED network. For reduced response times and for improved connectivity to hard-to-reach areas, such a network was seen as useful. The challenges identified include the operationalization of an autonomous AED drone network, privacy and security issues, existing legal and regulatory requirements, financial liabilities, public buy-in and public concern for the practical use of an AED, and the need for drone network therapy and cost-effectiveness research. The implementation facilitators for the AED drone network included strengthening key alliances (including integration into established EMS or fire services), finding viable private and public funding, and learning from existing drone models (e.g. commercial packages or distribution of medical supplies).
This study found general and conceptual support from a number of related fields for the creation of a drone network for AED delivery through key informants. In creating a regional drone AED network, such details should be considered.
Effect of Amplitude Spectral Area on Termination of Fibrillation and Outcomes in Pediatric Cardiac Arrest
Raymond T, presented a study at American Heart Association Scientific Sessions 2020: A Virtual Experience, which distinguished Amplitude Spectral Area (AMSA) from a collaborative pediatric resuscitation quality (pediRES-Q) during Pediatric Cardiac Arrest (pCA) and suspected that AMSA will be correlated with Termination of Fibrillation (TOF) and return of spontaneous circulation (ROSC).
Children below the age of 18 years with pCA and Ventricular fibrillation (VF) were examined. Prior to each shock, AMSA was measured for 2 seconds and also averaged for each subject (AMSA-avg). After defibrillation (DF), TOF was defined as termination of VF 10 secs at any rhythm other than VF.ROSC was defined as >20 minutes without chest compressions. Univariate and multivariate logistic regression tests were conducted to monitor weight, current and disease (cardiac vs non-cardiac) groups. TOF and ROSC with no Extracorporeal membrane oxygenation (ECMO) were the main endpoints. 24-hr survival and hospital discharge survival were secondary endpoints.
50 children from 14 hospitals (median age 3.7 years [IQR 0.6, 13.1]; median weight 16.3 kgs [IQR 6.9, 37.2]; 46 % male; 73 % category of heart disease) were found between 2015-2019. IHCA occurred in 47 and OHCA in 3 children, respectively. 111 shocks were analyzed with median DF 1.0 [IQR 1.0, 3.0], median DF energy 3.27 J/kg [IQR 2.65,5.01], median DF 0.64 A/kg [IQR 0.38,0.96], median AMSA 12.21 [IQR 7.17,17.03], and median AMSA-avg 14.6 [IQR 8.6,19.2]. TOF was reached in 72 DFs (65%), 31 (62%) in ROSC without ECMO, 11 (22%) in ROC with ECMO, 40 (80%) in 24-hour survival, and 26 (52%) in hospital discharge survival. Significantly correlated with TOF for the first shock is weight (OR 0.91 [0.84,0.99] p=0.025) and DF current (OR 1.44 [0.97, 2.2] p=0.07), but not AMSA. There was an important correlation between AMSA-avg (OR 1.11[1.0, 1.24] p=0.044) and ROSC without ECMO for DF current and illness category control. The relation between AMSA-avg and 24-hour survival or hospital discharge survival was not important.
TOF was associated with weight and DF current in pediatric patients but not AMSA, while AMSA-avg was associated with ROSC without ECMO but not 24-hour survival or hospital discharge survival.
Rapid Responder Operating Times for Out-of-hospital Cardiac Arrest Using Three Automated External Defibrillator Models
Gao M, presented a study at American Heart Association Scientific Sessions 2020: A Virtual Experience, which hypothesized the Rapid Responder Operating Times for Out-of-hospital Cardiac Arrest Using Three Automated External Defibrillator (AED) Models. Although simulation experiments were used to test usability factors for AED, the aim was to report the actual running time for three models of Philips AED used in sudden cardiac arrest (SCA) responses. From 2007 to 2018, a comfort dataset recorded by Philips AEDs (HS1, FRx, or FR3) was obtained from Europe and the United States. The FRx is for Basic Life Support (BLS), and the FR3 is for both BLS and Advanced Life Support (ALS) responders. The HS1 is intended for minimally trained or untrained individuals. To record the operating time intervals for cases where a shock was administered after initial rhythm analysis, a retrospective review was performed. There were 90 HS1, 46 FRx and 32 FR3 cases examined in the study.
Both FRx (p < 0.001) and FR3 (p = 0.001) respondents spent less time positioning the patient’s padson as expected after powering on the AED relative to HS1. Similarly, the time intervals for FRx (p = 0.02) and FR3 (p < 0.01) from the start of the shock recommended prompt to the first shock transmission are shorter than for HS1. In 74.4% (67 of 90) HS1 cases, 97.8% (45 of 46) FRx cases, and 100% (32 of 32) FR3 cases, the time from AED power-on to the first shock was within 90 seconds. On average, within 48 seconds, the FR3 and FRx responders were able to administer the first shock.
The analysis shows that despite different training levels, responders were able to quickly apply the AEDs and respond to the shock advisory prompt for all three AED models. However, this real-world output is better than most recorded simulation studies, but this study cannot express a spectrum of activities that account for timing variations (e.g. pads applied before power-on, or compressions started before pads were applied, etc.).
