Diabetes is the leading cause of CKD and kidney failure. ~40% of people with T2D develop CKD. The risk of CV mortality increases with increased CKD staging, regardless of diabetes status. Paola Fioretto assessed the role of GLP-1RAs in the CKD and T2D nexus. The findings were presented at the th st EASD Annual Meeting 2025, held from 15-19 September 2025 in Vienna, Austria
ADA recommendations include GLP-1RAs in people with high-risk T2D with CV or kidney disease. KDIGO supports the use of GLP-1RAs for people with CKD and T2D and/or obesity. Despite recent progress in the treatment of CKD, a considerable residual risk remains. FLOW trial enrolled predominantly a very high-risk CKD population based on the KDIGO criteria & Semaglutide 1.0 mg reduced the risk of first composite kidney event. There was 24% reduction in risk of composite kidney event. Semaglutide 1.0 mg slowed the loss of kidney function as measured by eGFR.
Semaglutide 1.0 mg reduced the risk of MACE and all cause death- 18% reduction in risk of MACE & 20% reduction in risk of all-cause death. Semaglutide 2.4 mg reduced the risk of kidney events in people with obesity and without T2D. Semaglutide benefits are independent of baseline BMI and not mediated by weight loss. In the SELECT trial, Semaglutide 2.4 mg reduced the risk of kidney events in people with obesity and without T2D.
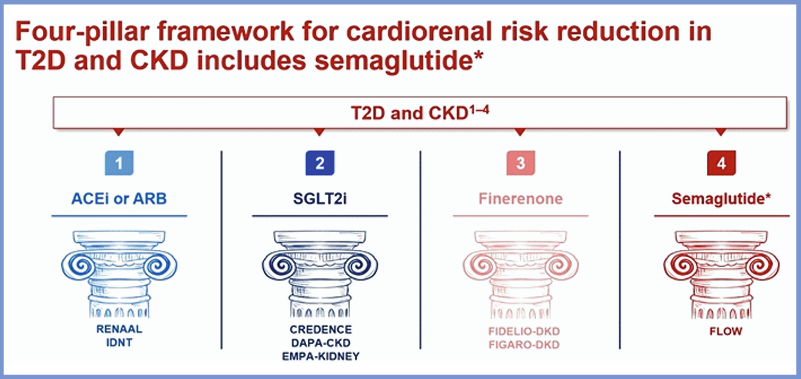
In the SMART trial, Semaglutide 2.4 mg reduced albuminuria in people with overweight or obesity and CKD without diabetes with 52% reduction in UACR. The four-pillar framework for cardiorenal risk reduction in T2D and CKD includes semaglutide. The actuarial analysis of kidney outcomes trials indicate that combination therapies may have potential benefits on CKD progression.
About 40% of people with T2D develop CKD, which is associated with an increased risk of CVD. Current guidelines for the management of CKD in people with T2D recommend use of GLP-1RAS. Kidney protection needs a multi-target treatment approach to slow disease progression and CVD risk. OW s.c. semaglutide 1.0 mg improves kidney and CV outcomes in people with CKD and T2D4. OW s.c. semaglutide 2.4 mg improves kidney and CV outcomes in people with overweight and obesity.
