Oyewole OM, et al. Iranian J Nursing Midwifery Res 2020;25:58-64.
Oyewole OM, et al., conducted a study to investigate the potency of a training programme on knowledge and practice of lifestyle modification within hypertensive patients.
A quasi‑experimental design was performed with accidental sampling to choose the sample size (n = 30). The World Health Organization (WHO) and Hypertension Knowledge‑Level Scale (HK‑LS), revised organized questionnaires to determine knowledge of hypertension, lifestyle modification and practice. Using the statistical package for the social science software, tables, percentages, mean, standard Deviation and t‑test were used for data analysis at 0.05 levels of significance.
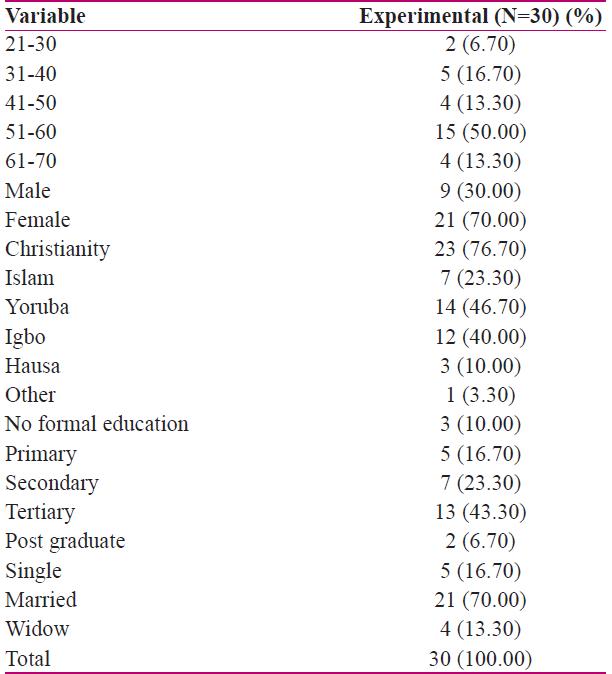
A greater percentage of the participants were female (70.00%) and Christians (76.70%) in the groups (Table 1).
Table 1: Socio‑demographic data of Hypertensive Patients Attending out‑Patient Clinics in Lagos, Nigeria
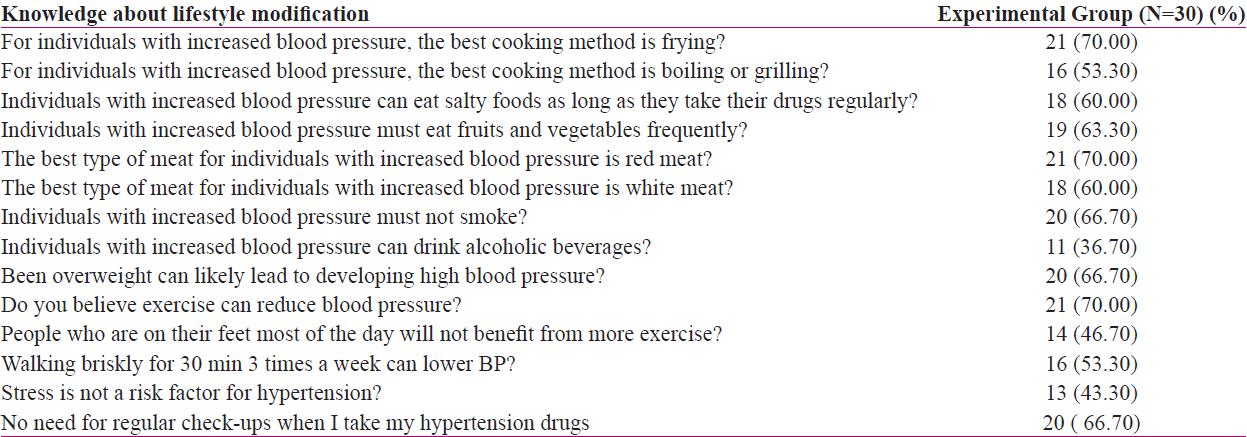
It was identified that 70% in the group responded that the best cooking method is not frying, 53.30% in the group responded the best method is boiling or grilling and 60% responded that subjects with hypertension should not eat too much salt even if they are on medicines (Table 2).
Table 2: Pre intervention knowledge about lifestyle modification among Hypertensive Patients Attending out‑Patient Clinics in Lagos, Nigeria
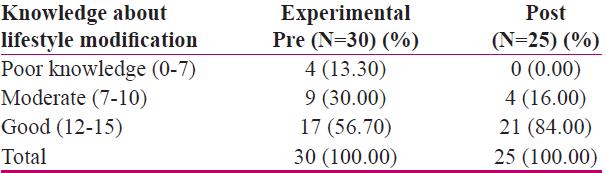
It was identified that 56.70% offer good knowledge regarding lifestyle modification pre‑test and 80% offer good knowledge regarding lifestyle modification following the training programs. Whereas, 13.30% offer poor knowledge pre‑test and poor knowledge, which is entirely removed following the application of training program (0%) (Table 3).
Table 3: Summary of responses on knowledge about lifestyle modification pre intervention
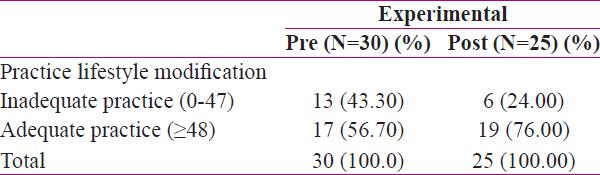
After the application of the training program, it was observed that increase in practice (adequate ≥41) from 56.70% to 76% at the experimental group which is comparatively high when the scores are comparing with each other. Inadequate practice (0‑47) reduced from 43.30% to 24% (Table 4).
Table 4: Summary of responses on practice of lifestyle modification post intervention
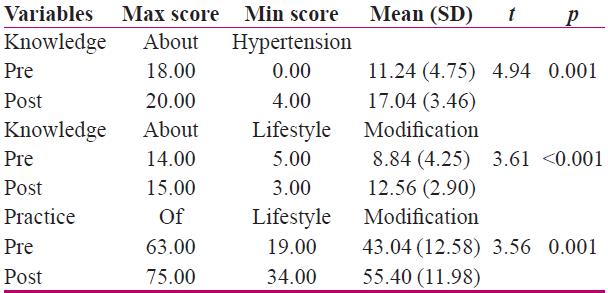
It was identified that the t‑test of the pre‑knowledge regarding hypertension within hypertensive subjects varied significantly from post‑knowledge following intervention (t=4.90, p=0.001). Furthermore, a significant difference was observed between the pre and post knowledge level regarding lifestyle modification following intervention (t=3.62, p=0.001). A significant difference was also found between the pre and post-practice of lifestyle medication after the intervention (t=3.56, p=0.001) (Table 5).
Table 5: t‑test analysis for knowledge and practice
Thus, the finding of this study offers evidence for responsiveness to modifying in knowledge and practice of life‑style modification following educational training was introduced. In this perspective, holding an educational training program is a primary tool that can be utilized to execute positive behavioural alterations required in the management of hypertensive subjects.
