Bouisset F, Ruidavets JB, Bongard V, Taraszkiewicz D, Bérard E, Galinier M, et al. Long-term Prognostic Impact of Physical Activity in Patients With Stable Coronary Heart Disease. Am J Cardiol. 2020 Jan 15;125(2):176-181.
Physical activity (PA) is part of cardiac rehabilitation program which demonstrates to reduce cardiovascular mortality and hospital admission in Coronary Heart Disease (CHD) patients. Current European guidelines for management of stable CHD patients recommend to practice a regular physical activity consisting of 30 minutes of moderate-to-vigorous intensity aerobic exercising, at least 3 times a week. The American guidelines encourages CHD patients to practice 150 minutes per week of moderate intensity exercising, both for primary and secondary prevention. Bouisset F, et al., conducted a study to evaluate the impact of physical activity level on mortality at long term in stable CHD patients.
A total of 822 patients with stable CHD were enrolled in the study. PA was evaluated by the MOSPA questionnaire. PA was expressed in weekly metabolic equivalent scores (MET) hour per week and for the present analysis, PA was graduated in tertiles and the cohort was thus divided into three groups. Three tertiles of patients were individualized: 0.0-9 Metabolic Equivalent of Task (METs) hour per week (n = 267); 10-39.9 METs hour per week (n = 279); and ≥40 METs hour per week (n = 276). After a median follow-up of 14.6 years, 324 patients had died. In a multivariate analysis adjusted for age, dyslipidemia, smoking status, diabetes, high blood pressure, waist circumference, left ventricular ejection fraction, Gensini score, heart rate, ankle-brachial index and duration of disease, physical activity was significantly and independently associated with all cause mortality. At the end of the follow-up period, mortality rate was 46.1% in the lowest tertile, 23.4% in the median, and 17.6% in the highest (log rank test, p <0.001) (Figure 1).
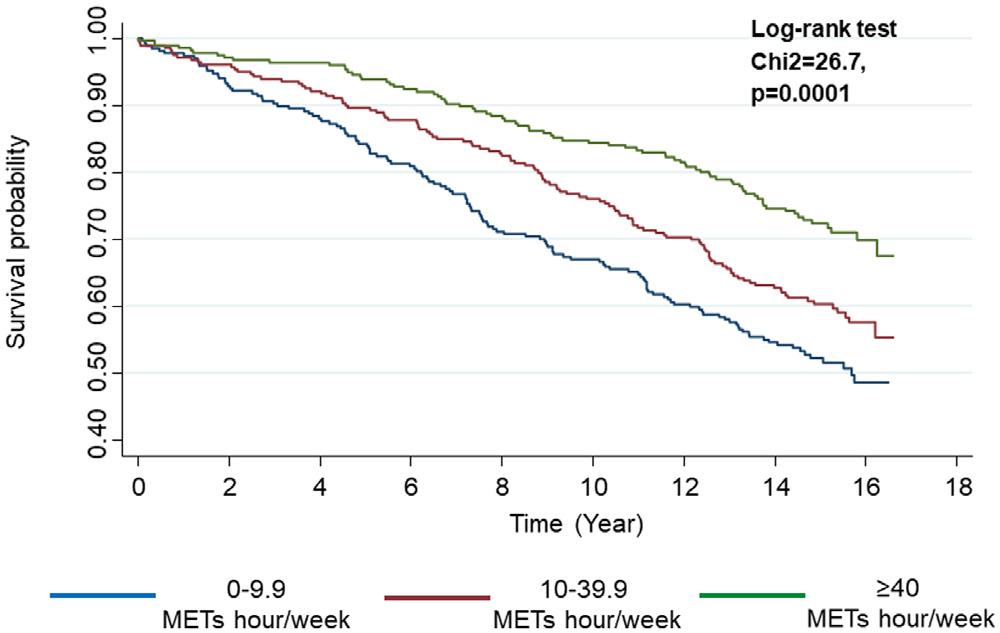
Figure 1: The Kaplan-Meier cumulative survival curves, according to PA
Compared to the first tertile (0 to 9.9 METs hour per week), both the second tertile (10 to 39.9 METs hour per week) and the third tertile (>40 METs hour per week) were associated to a reduction of all-cause mortality risk with HR at 0.79 (95%CI [0.61:1.03], P = 0.08) and 0.71 ([0.53:0.96], P = 0.025) respectively; P for trend = 0.02. Adjusted hazard ratios for an increase of 10 METs hour per week was 0.95 [0.92 to 0.98], (P <0.002) (Table 1).
Table 1: Multivariable Cox regression or the association between levels (tertiles) of physical activity and all-cause of death

Thus, the study demonstrates an independent association between PA and long term vital prognosis with a 5% total mortality decrease for an increase of 10 METs hour per week.
