Khurshid S. Eur Heart J. 2021 Jul 1;42(25):2472-2483.
Physical activity has long been implied as an atrial fibrillation (AF) risk factor, however associations among activity and AF have been different and based largely on self-report. Most population-based studies have detected decreased AF risk with exercise. Yet there may be limited advantages to those participating in vigorous activity, and may be confused by body mass index. Khurshid S, et al. conducted a study which evaluated correlations among physical activity and incident AF and stroke, assuming that individuals meeting guideline-based activity recommendations would have a decreased risk of incident AF and stroke following adjustment for AF risk factors.
The UK Biobank is a prospective group of 502,629 participants enlisted in 2006–2010. 7000 patients from103,695 participants contributing accelerometer data, were excluded for insufficient wear time or failure of calibration, 281 with insufficient data for clinical AF risk assessment, and 2745 with prevalent AF, withdrawn consent, or absence of follow-up data, resulting in 93,669 individuals in the primary examination. The primary outcome was incident AF. Atrial flutter was considered equivalent to AF. Given the significance of stroke as a contributor to AF correlated morbidity, incident stroke was analysed as a secondary outcome. Whether measured activity met the standard recommendations of the European Society of Cardiology, American Heart Association, and World Health Organization [moderate- to-vigorous physical activity (MVPA) ≥150 min/week] were classified. Cox proportional hazards models adjusted for age, sex, and each component of the Cohorts for Heart and Aging Research in Genomic Epidemiology AF (CHARGE-AF) risk score was used to analyse correlations among guideline-adherent activity and incident AF (primary) and stroke (secondary). An association among accelerometer-derived and self-reported activity was also evaluated.
The mean age of patient was 62± 8 years and 57% were female. In total, 2338 patients had incident AF across a median of 5.2 (quartile-1: 4.6, quartile-3: 5.8) years of follow-up spanning. In multivariable adjusted models, guideline-adherent activity was correlated with decreased risks of AF [hazard ratio (HR) 0.82, 95% confidence interval (CI) 0.75–0.89; incidence 3.5/1000 person-years, 95% CI 3.3–3.8 vs. 6.5/1000 person-years, 95% CI 6.1–6.8] and stroke (HR 0.76, 95% CI 0.64–0.90; incidence 1.0/1000 person-years, 95% CI 0.9–1.1 vs. 1.8/1000 person-years, 95% CI 1.6–2.0). (Figure 1) (Table 1)
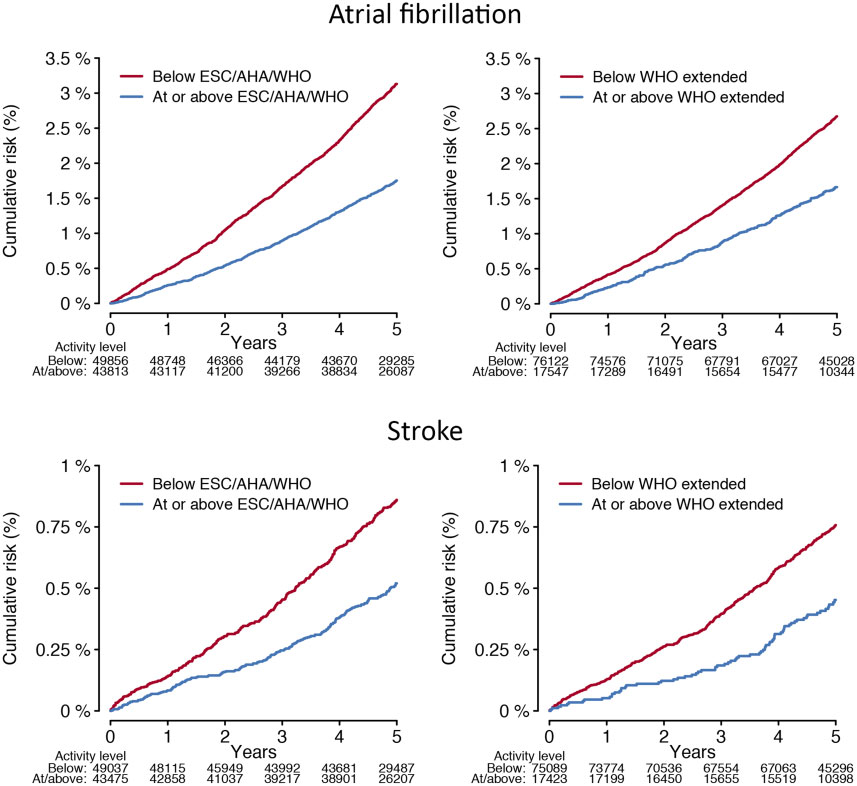
Figure 1: Cumulative risks of atrial fibrillation and stroke stratified by adherence to physical activity recommendations.
Depicted is the cumulative risk of atrial fibrillation (upper panels) and stroke (lower panels) stratified by accelerometer-derived physical activity levels meeting European Society of Cardiology, American Heart Association, and World Health Organization standard thresholds (≥150min of moderate-to-vigorous physical activity per week, left panels), and the World Health Organization threshold for additional health benefits (≥300min of moderate-to-vigorous physical activity per week, right panels).
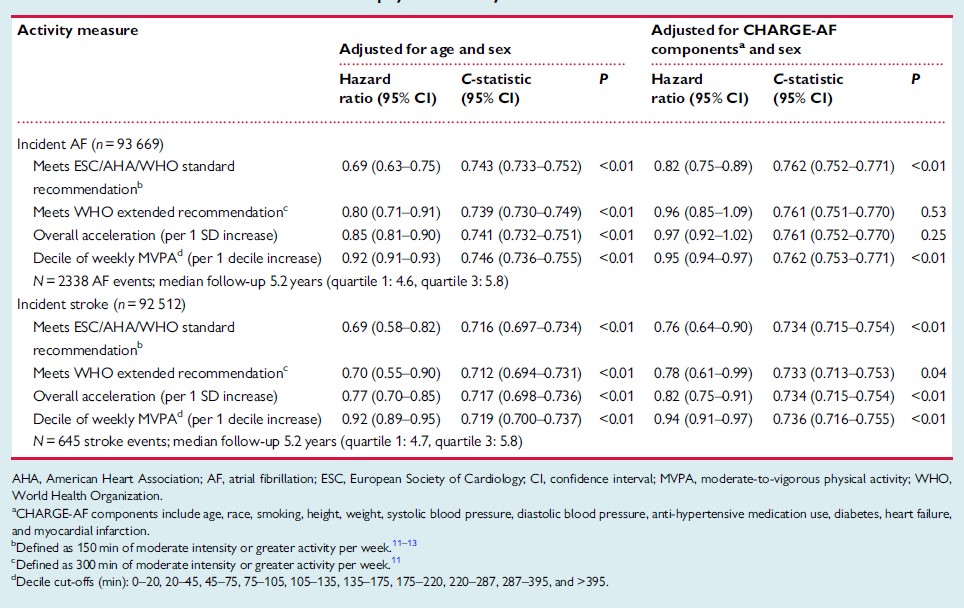
Table 1: Multivariable associations between physical activity and incident atrial fibrillation and stroke
An association among accelerometer-derived and self-reported MVPA was weak [r= 0.16 (95% CI 0.16–0.17), p< 0.0 Self-reported activity was not correlated with incident AF or stroke (Figure 2).
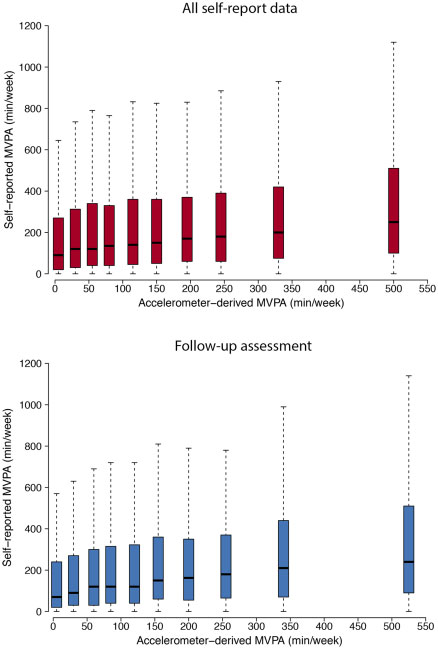
Figure 2: Distribution of self-reported moderate-to-vigorous physical activity across deciles of accelerometer-derived moderateto- vigorous physical activity. Depicted are distributions of self-reported moderate-to-vigorous physical activity (y-axis) across deciles of increasing accelerometer-derived moderate-to-vigorous physical activity (x-axis).
Each boxplot represents a decile of accelerometer- derived moderate-to-vigorous physical activity and is located at the median accelerometer-derived moderate-to-vigorous physical activity within that decile. For each boxplot, the black bar denotes themedian self-reportedmoderate-to-vigorous physical activity, the box represents the interquartile range, and the whiskers represent points beyond the interquartile range. The top plot depicts all 93 579 individuals contributing self-report data (median [quartile 1, quartile 3] years from questionnaire to accelerometer wear 5.5 [4.6, 6.3]), while the bottom plot depicts 8205 individuals contributing self-report data at a follow-up assessment (2.2 [1.8, 2.5]). Points greater than quartile 3 plus 1.5 times the interquartile range and points smaller than quartile 1 minus 1.5 times the interquartile range are not depicted
Graphical Abstract
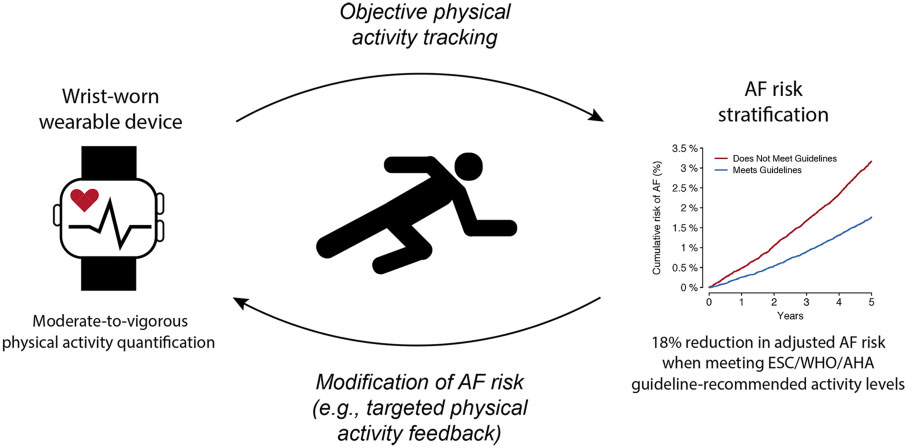
It was concluded that higher accelerometer-derived physical activity is correlated with decreased risks of AF and stroke. Future preventive efforts may be most efficacious to decrease AF risk while targeting adherence to aim activity thresholds.
