Son M. PLoS One. 2020 Feb 14;15(2):e0228684.
Serum uric acid levels are known to be highly associated with stroke, coronary artery disease as well as hypertension and metabolic syndrome. But, the certain role of serum uric acid is not yet authenticated in these disorders, because of its correlation with numerous other risk factors such as diet, obesity and dyslipidemia. In the community, information on the correlation of dyslipidemia with serum uric acid is insufficient regardless of the high prevalence (11.4%) of hyperuricemia in Korean population. Contemplating the results of the aforementioned studies being deficiently adjusted for the various laboratory & clinical confounders, Son M. et al., conducted a study to analyse the independent association among individual components of dyslipidemia and serum uric acid, with the representative datasets of the Korean population, using extensive adjustments for possible confounders.
This study examined data from the seventh KNHANES, a cross-sectional survey. 8,722 (male 3,704 [42.4%]) participants over the age of 19 without missing values were evaluated from the total number of 16,277 participants. In a group of a total 8,722 participants, 1,061 participants were recognized as the hyperuricemia group (prevalence 12.2%, uric acid level assigned as ≥7 mg/dL in men, ≥6 mg/dL in women) whereas 7,661 participants were delegated to non-hyperuricemia group. A sexual proportion (male to female); BMI; waist circumference; SBP and DBP; haemoglobin; BUN; GFR; high sensitivity C-reactive protein; and serum uric acid levels were increased in the hyperuricemia group whereas average age was lower as compared to non-hyperuricemia group. Total cholesterol, triglycerides, LDL-C and non-HDL-C levels were increased although serum HDL-C levels were reduced with hyperuricemia. In the hyperuricemia group, participants with elevated cumulative numbers of dyslipidemia components were substantially prevalent (p < 0.001).
Serum uric acid levels exhibited positive trend (or negative trend with HDL-C) within each components of dyslipidemia (p < 0.001) excluding LDL-C (p = 0.021) after adjusting for age, sex, waist circumference, BMI, haemoglobin, BUN, GFR, hypertension, diabetes, smoking status, consumpation of alcohol, regular exercise and the regulation of dyslipidemia medication (model 4) (Figure 1).
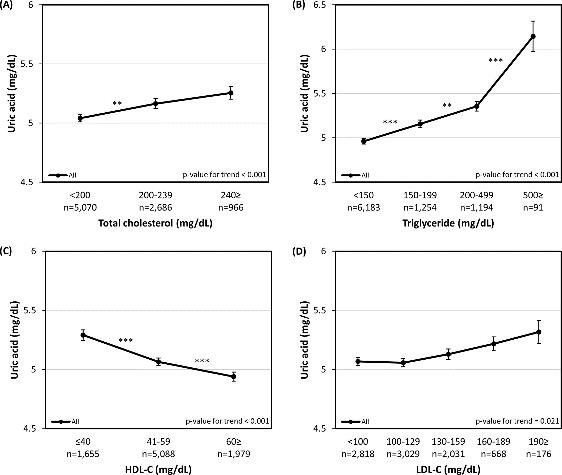
Figure 1: Adjusted serum uric acid levels according to the individual dyslipidemia components. (A) Total cholesterol (B) Triglyceride (C) HDL-C (D) LDL-C
Adjusted serum uric acid levels exhibited a tendency to enhance collaterally with the elevating number of dyslipidemia components, with each statistically substantial comparison except with the one among components of 2 and 3≥ (p = 0.729) from the all participants group (Figure 2A). The uric acid level was substantially decreased in the categories of 1 dyslipidemia component and the 3≥ dyslipidemia components in the medication administrated group (p< 0.05, p< 0.001, resp.) (Figure 2B).
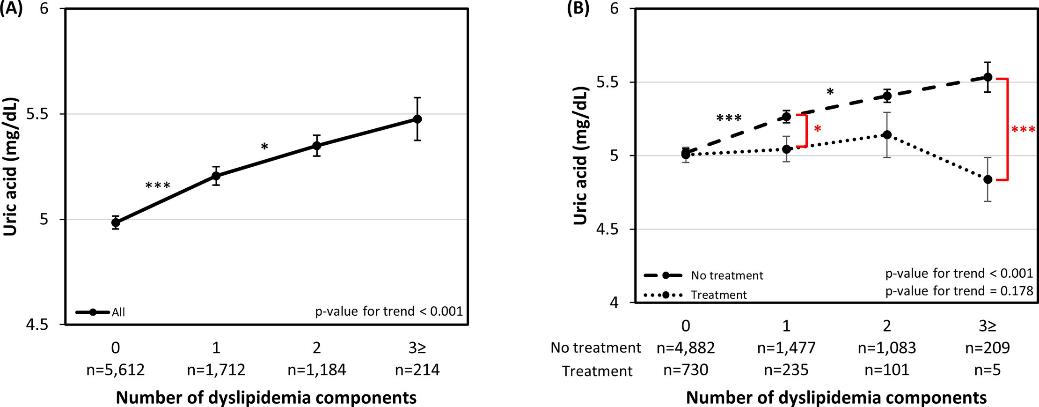
Figure 2: Adjusted serum uric acid levels according to the number of dyslipidemia components. (A) All participants, Adjusted for age, sex, waist circumference, BMI, hemoglobin, BUN, GFR, HTN, DM, smoking, alcohol consumption, regular exercise and dyslipidemia medication (B) Dyslipidemia medication administered group and non-administered group, Adjusted for age, sex, waist circumference, BMI, hemoglobin, BUN, GFR, HTN, DM, smoking, alcohol consumption and regular exercise
Individual components of hypercholesterolemia (p < 0.001), hypertriglyceridemia (p < 0.001) and HDL-C (p < 0.001) possessed substantial associations with hyperuricemia after further adjusted for the components combined. In addition, when non-HDL-C was replaced with total cholesterol non-HDL-C (p < 0.001) exhibited a substantial correlation with hyperuricemia.
Thus, it was concluded that the dyslipidemia components of serum total cholesterol, triglycerides and LDL-C levels are positively correlated with serum uric acid levels, although serum HDL-C levels are conversely associated. To confirm the accurate correlation among dyslipidemia and serum uric acid levels, further complementary studies concerning other lipid parameters are required.
KNHANES: Korea National Health And Nutrition Examination Survey; BMI: Body mass index; SBP: Systolic blood pressure; DBP: Diastolic blood pressure; BUN: Blood urea nitrogen; GFR: Glomerular filtration rate; LDL-C: Low density lipoprotein cholesterol; HDL-C: High density lipoprotein cholesterol; HTN: Hypertension; DM: Diabetes mellitus
