Duca LM. Am Heart J. 2020 Mar;221:95-105.
Congenital heart defects (CHDs) surround any gross structural abnormality of the heart or intrathoracic great vessels present at birth. The judging of infant CHD prevalence assesses to adulthood may be incorrect since individuals diagnosed at birth may go through multiple procedures in infancy for survival, while others, asymptomatic in childhood, shows symptoms at an older age. Surveillance systems progressed with EHR data frequently fail to capture all entitled cases because of restrictions in case determination procedures, individuals with a CHD were recognized from multiple, unrelated electronic data sources by Colorado Congenital Heart Disease (COCHD) surveillance system. It was pivotal to recognize individuals from the target population not captured by our primary case-finding data sources to enhance the certainty of the COCHD population-based prevalence estimates. A capture-recapture procedure was used to estimate prevalence of undetected or missed individuals. To date, this method is more accurately evaluate the prevalence of a variety of conditions, inclusive of intussusception after rotavirus vaccination, tuberculosis, meningococcal disease, diabetes and CHDs between infants and children. Duca LM et al., conducted a study to evaluate the prevalence of CHDs between adolescents and adults in Colorado with capture-recapture methodology over incomplete case ascertainment.
A 3-year study period (January 1, 2011 to December 31, 2013) data was used by the COCHD surveillance system, a statewide population based surveillance system included adolescents and adults from Colorado with a diagnosis of a CHD. If individuals had a CHD lesion listed as an encounter diagnostic code, in co-occurrence with being age eligible (11-64 years) and living in the state of Colorado, at any time in the 3 years were incorporated in the COCHD surveillance system. The surveillance system was established over the combination of multiple pre-existing electronic health records (EHR) and health insurance claims data in Colorado. Capture-recapture analyses were executed with the five primary case-finding data sources to measure the prevalence of CHDs in adolescents and adults in Colorado, adjusted for incomplete case ascertainment. An age (dichotomized into adolescents [age 11-17] and adults [age 18- 64]), CHD severity (dichotomized into severe and mild/moderate), and health insurance status were assessed as prospective origins of heterogeneous capture probability by testing for a correlation among these variables and recognition over case recognizing data sources with a chi-squared test.
In all data sources, a total of 16,480 individuals recognised, 12,293 unique adolescents and adults with CHDs were recognised by at least one of the five case-finding data sources. Overall, 8,983(73.1%) individuals were recognized in only one data source, 2,872 (23.4%) in two data sources, 421 (3.4%) in three data sources, 17 (0.1%) in four data sources, and none in all five data sources. 10,934 (89%) had mild to moderate and 1,359 (11%) had severe CHDs between all individuals.
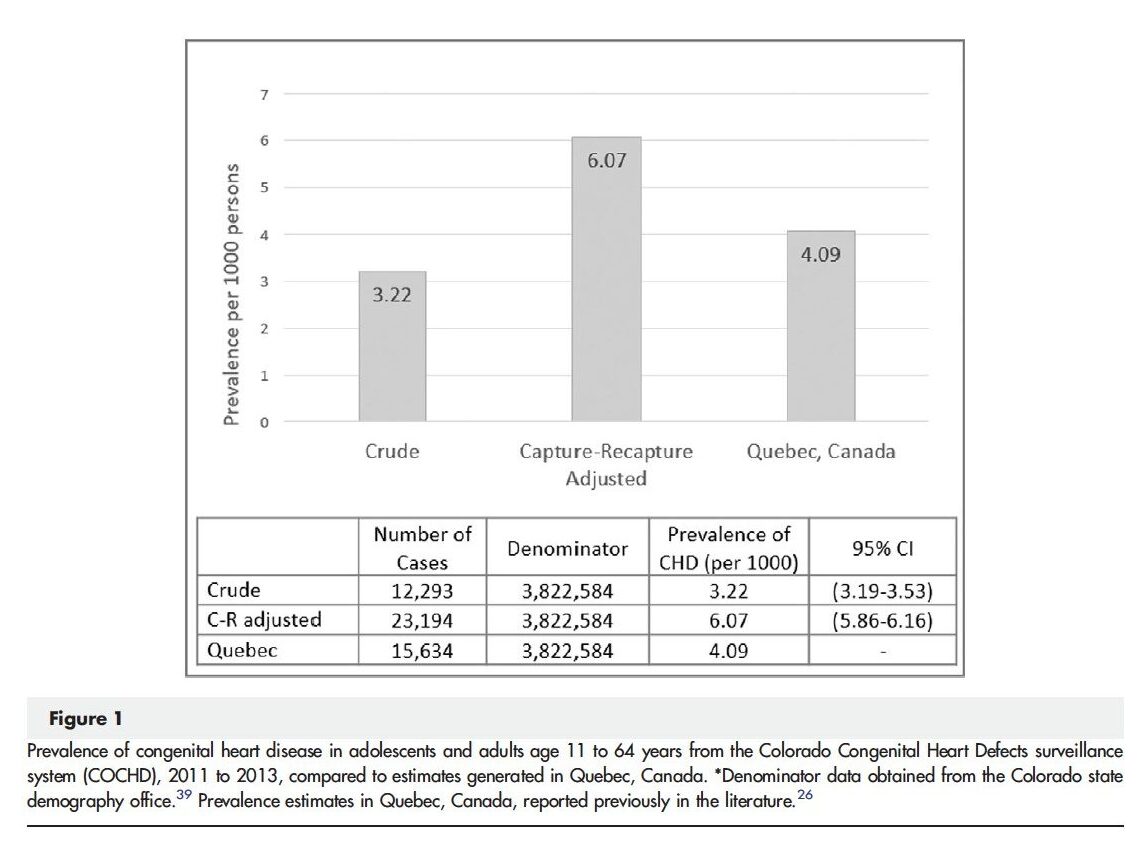
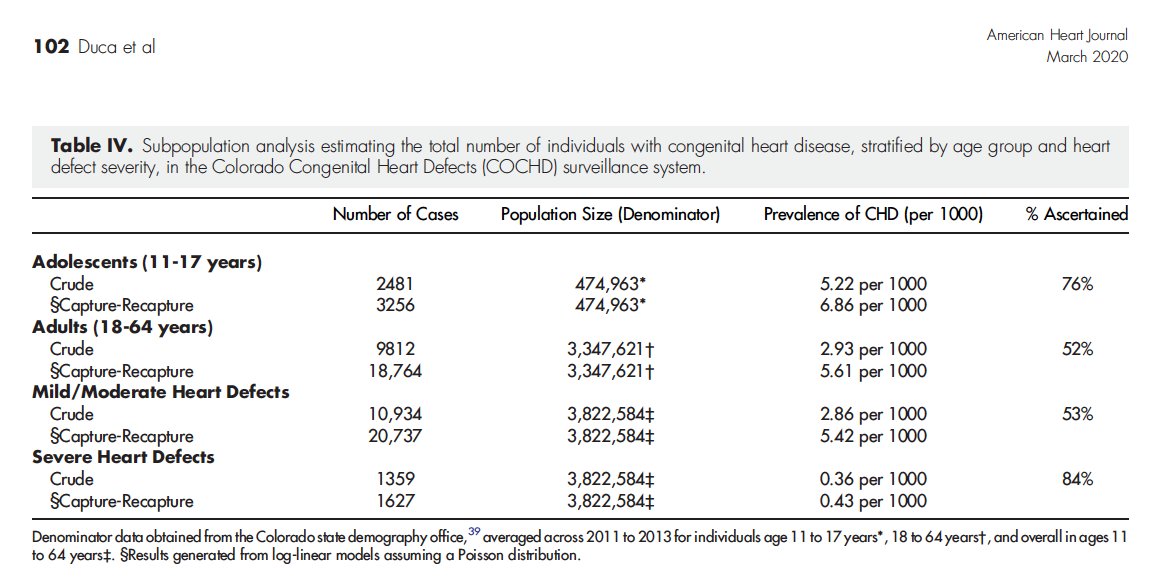
A substantial correlation was found among defect severity and recognition in multiple case-identifying data sources (p<.0001). In addition, 2,481 (20%) individuals with a CHD were age 11-17 years and 9,812 (80%) were 18-64 years. A substantial correlation was found among recognition in multiple case identifying data sources and age group (p<.0001), as well as health insurance status (p<.0001), showed heterogeneous capture probability by age group, defect severity, and health insurance status. The crude prevalence estimate of CHDs gained from the COCHD surveillance system was 3.22 per 1000 individuals aged 11-64 years [(12,293/3,822,584) x 1000] in adolescents and adults. The capture-recapture adjusted prevalence estimate was 6.07 per 1000 individuals aged 11-64 years, showed 47% of the cases were not recognised in the case identifying data sources in the catchment area. (Figure 1), In adolescents (n=2,481), the capture-recapture methodology showed a corrected total population size of 3,256, exhibited 24% of adolescents with a CHD were missed in the surveillance system. (Table 1)
Thus, it was concluded that a new information on the prevalence of CHDs in adolescents and adults was shown in this statewide study. These high prevalence rates highlighted the requirement for additional specialized care facilities for this population with CHDs.