Why Precision Medicine is The Future Of Diabetes Medicine
Udler M, presented the first topic “Why precision medicine is the future of diabetes medicine” from the session “EASD/ADA Symposium: Optimising Diabetes Diagnosis, Prevention And Care: Is Precision Medicine The Answer” on 29th September 2021.
Precision medicine aims to deliver the right treatments in the right dosage at the right time –every time. With the global diabetes prevalence rising rapidly, it is crucial to have ideal screening practices and management for at-risk patients with diabetes. As per CDC, around 90% of diabetes patients don’t know they are diabetic. There is a possibility of few patients having cure or remission. However, glycaemic targets are met by <50% of patients adherent to medications. Moreover, majority of people develop worsening beta cell function despite treatment. Hence, it is imperative to identify high-risk individuals and determine the intervention for precision prevention. Depending on definition, around 30% population may have prediabetes. Approxiamtely 5-10% are expected to progress to T2D each year and upto 59% of people diagnosed with prediabetes may spontaneously return to normoglycemia within 1-5 years of follow-up. As per a study conducted by Ahlquvist, patients were stratified into five subgroups with differing disease progression and risk of diabetic complications. This new substratification might eventually help to tailor and target early treatment to patients who would benefit most, thereby representing a first step towards precision medicine in diabetes.
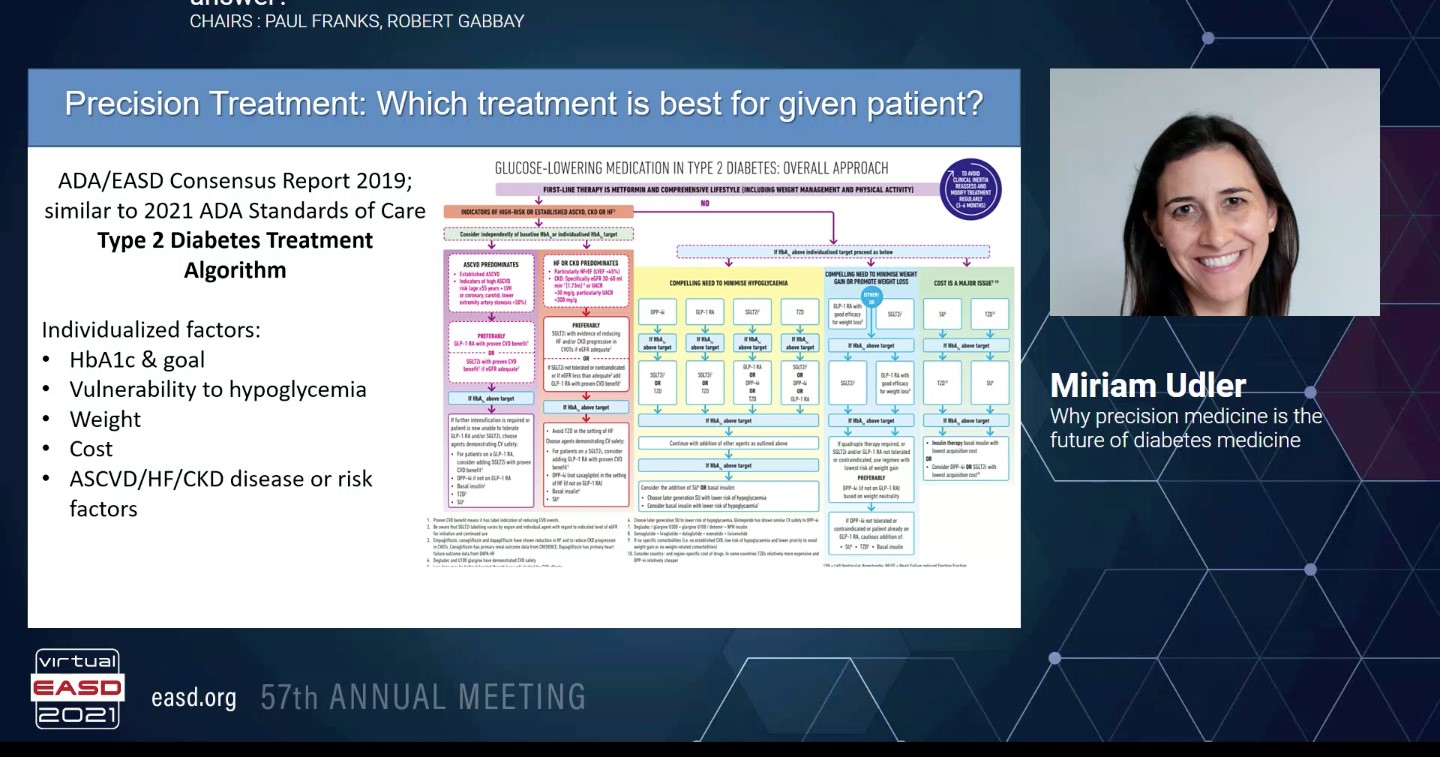
Diagnostic uncertainty may still remain despite a battery of tests. Type 1 diabetes needs to be differentiated from type 2, MODY, and monogenic autoimmune diabetes. For initiating the precision treatment, ADA/EASD Consensus report 2019 which is similar to 2021 ADA standards of care type 2 diabetes treatment algorithm considers individualized factors like HbA1c and goal, vulnerability to hypoglycrmia, weight, cost, ASCVD/HF/CKD disease or risk factors. However, simple individual-level traits (sex, age of diagnosis, baseline BMI and HbA1c) predicted response better than clusters in the initial step towards precision treatment. To understand the precision prognosis, it is important to ascertain the expected disease course and the increased risk of any complications or co-morbidities.
Precision medicine certainly needs to be the future of diabetes medicine because in current practice, the method of screening, recognising the subtype of diabetes and management of diabetes remains suboptimal. Moreover, there is a critical need for truly preventative, disease-modifying, and/or curative treatments. The mission of precision medicine is to treat the cause of disease rather than the symptom which requires better understanding of the disease pathways, refined disease classification and a framework for developing novel, mechanism-directed, and patient-centered therapeutic approaches.
CGM Detected Hypoglycaemia: What Is Its Clinical Relevance?
Iqbal A, presented a session on “CGM detected hypoglycaemia: What is its clinical relevance?” on 29th September 2021.
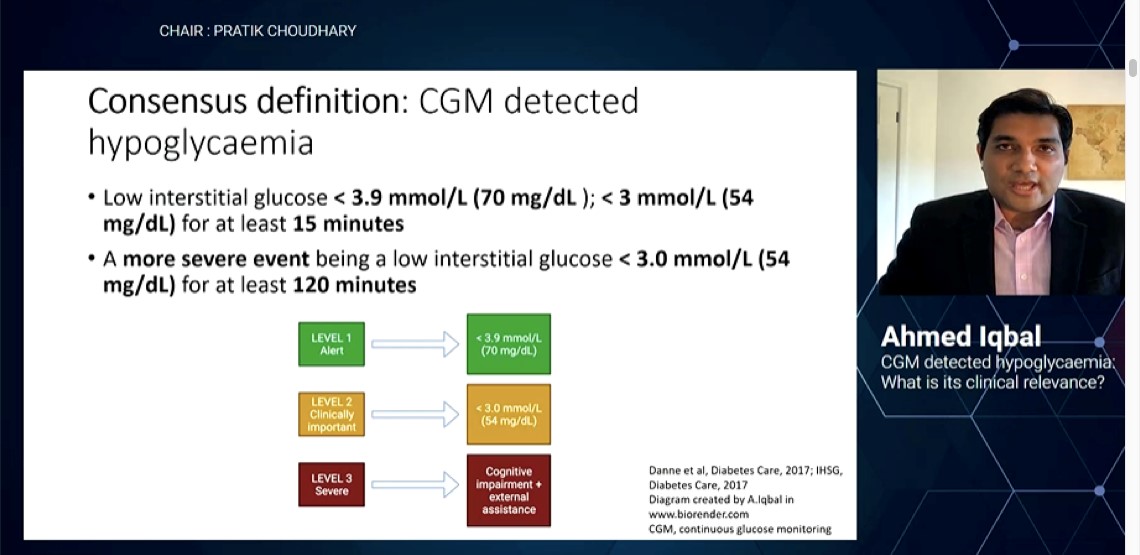
As per the consensus definition, continuous glucose monitoring (CGM) detected hypoglycaemia includes low interstitial glucose <3.9 mmol/L (70 mg/dL); <3 mmol/L (54 mg/dL) for atleast 15 minutes. A more severe event being a low interstitial glucose <3 mmol/L (54 mg/dL) for atleast 120 minutes. CGM monitoring allows to take steps in self-management as it is comprehensive, it optimises treatment, helps to understand the daily glucose trends, sets the alarms and facilitates lifestyle modification.
There are certain limitations when interstitial glucose (IG) is compared to capillary blood glucose (CBG) such as physiological lag between IG and CBG; under steady state for 4 to 10 mins and more when blood glucose falls rapidly. Also, when in studies CGM reported 19% higher glucose under hypoglycaemia and 8% higher under euglycaemia suggesting the limitation of CGM in detecting accurate period of hypoglycaemia.
Unfortunately, no randomised trials have shown that CGM use can reverse impaired awareness of hypoglycaemia (IAH). Use of CGM for > 6 months in IAH is still associated with upto 6 fold increased risk of severe hypoglycaemia.
As per a study conducted in healthy volunteers, hypoglycaemia causes inflammation and thrombosis. In patients with type 2 diabetes, inflammation and thrombosis can last upto 7 days. In summary, clinical use of CGM reduces hypoglycaemia in T1D and T2D. CGM accuracy in hypoglycaemia is a limitation and use of CGM does not appear to reverse IAH.
Future perspectives involves correlating CGM detected hypoglycaemia (symptomatic and asymptomatic) with patient reported outcomes; need for robust prospective data on CGM detected hypoglycaemia and clinical outcomes; and to explore the consequences of hypoglycaemia using CGM devices.
Hypoglycaemic Unawareness: Strategies to Prevent and Manage it?
Amiel S, presented a session on “Hypoglycaemic unawareness: Strategies to prevent and manage it” on 29th September 2021.
Impaired awareness of hypoglycaemia is defined as loss of subjective awareness of hypoglycaemia and a diminished ability to perceive the onset of hypoglycaemia.
Hypoglycaemia is seen in around 25-40% of people with type 1 diabetes, 10% of people with insulin treated type 2 diabetes. Hypoglycaemia increases the risk of severe hypoglycaemia by 6 to 17 fold. It is also associated with delayed and reduced stress response, which is inducible by level 2 hypoglycaemia and restorable by avoidance of level 2 hypoglycaemia.
The only way hypoglycaemia awareness can be restored is by hypoglycaemia avoidance. Before implementing diabetes technologies in treatment, insulin therapies should be optimized.
To prevent hypoglycaemia, one needs to first ask the patient about hypoglycaemia. Various patient tools and score cards can help to assess the hypoglycaemia. These scores and tools include the GOLD score, Clarke score, DAFNE tool, Pedersen-Bjergaard score. The next step is to check the blood glucose records and subsequently check with the family members.
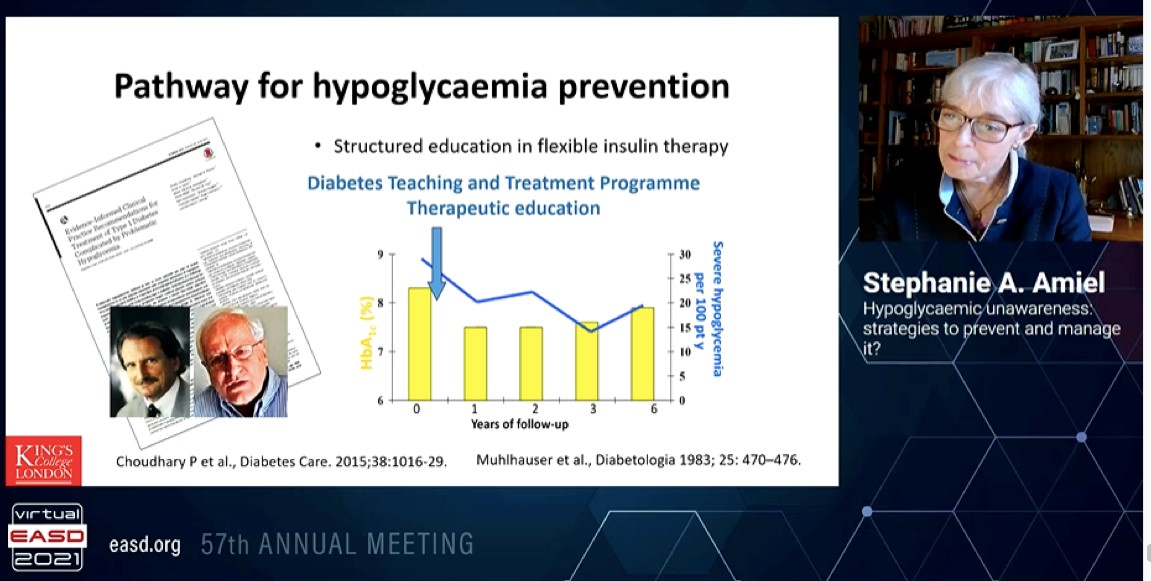
Blood glucose awareness training is a psychoeducational program. Mühlhauser et al. demonstrated that intensified insulin therapy, when combined with a 5-day teaching program, improved glycaemic control without increasing severe hypoglycaemia.
The pathway for hypoglycaemia prevention involves a structured education in flexible insulin therapt and incorporaton of diabetes teaching and treatment programme therapeutic education as patient education in diabetes has become an integral part of diabetes management.
Diabetes Democracy through Digital Patient Education and Training
The pandemic has presented unique challenges for people with diabetes, who comprise a high-risk group for severe COVID-19 infection. There has been increased emphasis on the importance of self-care activities for people with diabetes to optimise their diabetes management; however this has proven difficult because of restrictions due to lockdown and reduced face-to-face diabetes education. Gupta A, presented a study in a session at Virtual EASD Annual Meeting 2021 on 29th September 2021 which explored the impact of digital led patient education and training on the diabetes care.
A systemic review was done of the published evidence for implications of virtual patient education and training in diabetes during COVID-19 era, by searching pubmed-medline, Cochrane library, online databases. Data were analysed using meta-aggregation for the studies conducted till Sept 2020.
1008 patients were of T2DM and 91 were of T1DM. The virtual education and training occurred through telephone, zoom video conferencing app and Medtronic carelink system. The mean impact factor of the journals publishing these studies was 2.8. Prospective study was conducted in 3 phases: before education, after education and in the period of pandemic. Diabetics on oral therapy were included in the study. HbA1c was significantly higher before education compared to post education in COVID-19. BMI was significantly lower after education while QOL was substantially lower in all domain of COVID-19. HCL systems allows T1D patients to improve time in rang (TIR), time below range (TBR), and glycemic variability independently of previous treatment.
Virtual education and training are useful during pandemic that necessitates limiting the access of patients for in person follow up and yet, improving the continuity of care. Digital database intervention for patient education has the potential to translate democratization of diabetes care and enable access to care.
Diabetes Complications among Patients from Metropolitan versus Non-metropolitan Cities in India: One Year Results of LANDMARC
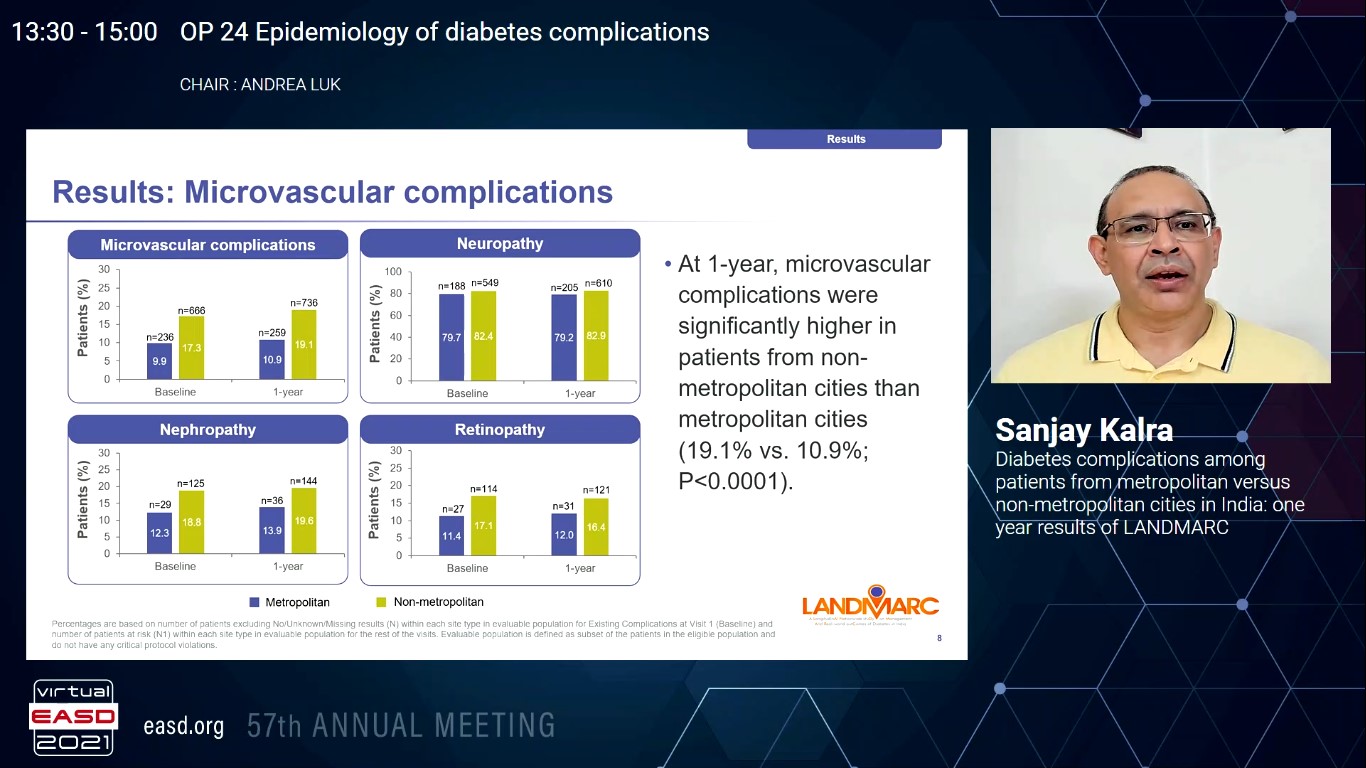
As type 2 diabetes (T2D) develops, it imposes damage to the vasculature. Micro- and macro-vascular complications are the vital reasons of morbidity and mortality correlated with T2D. In India, data are very limited on complications in patients with diabetes from metropolitan and non-metropolitan cities. Hence, Kalra S, presented a study in a session at Virtual EASD Annual Meeting 2021 on 29th September 2021 which evaluated micro- and macro-vascular complications in patients from metropolitan versus non-metropolitan cities in the first year of LANDMARC, a 3-year nationwide prospective observational study.
LANDMARC is the first nation-wide, prospective, long-term, multicenter, observational, and longitudinal study incorporating patients with T2D. Patients with T2D who were on ≥2 antihyperglycemic medications were included in the LANDMARC study. Each participant is aimed to be analysed across the 3-year period (March 2018 to March 2021), incorporating 7 visits at 6-months interval.
From the total 6236 enlisted patients, 2378 and 3858 were from metropolitan and non-metropolitan cities, respectively. Age, duration of T2D, and baseline A1C were alike over groups. At 1-year, patients from non-metropolitan showed substantially greater microvascular complications than metropolitan cities (19.08% vs. 10.89%; p<0.0001) (Table). Neuropathy was the most frequent microvascular complication shown in both the groups. Participants from non-metropolitan cities had higher macrovascular complications; and acute coronary syndrome and heart failure were the most frequent.
The present, first-of-its-kind data from India exhibited patterns of disease development between patients with T2D. Findings from this ongoing study showed that patients from non-metropolitan cities may have greater complications, especially microvascular.
Associations Between Chronic Kidney Disease, Prior Cardiovascular Conditions and Increased Mortality in 36.303 Type 1 Diabetes Patients Between 2015-2017
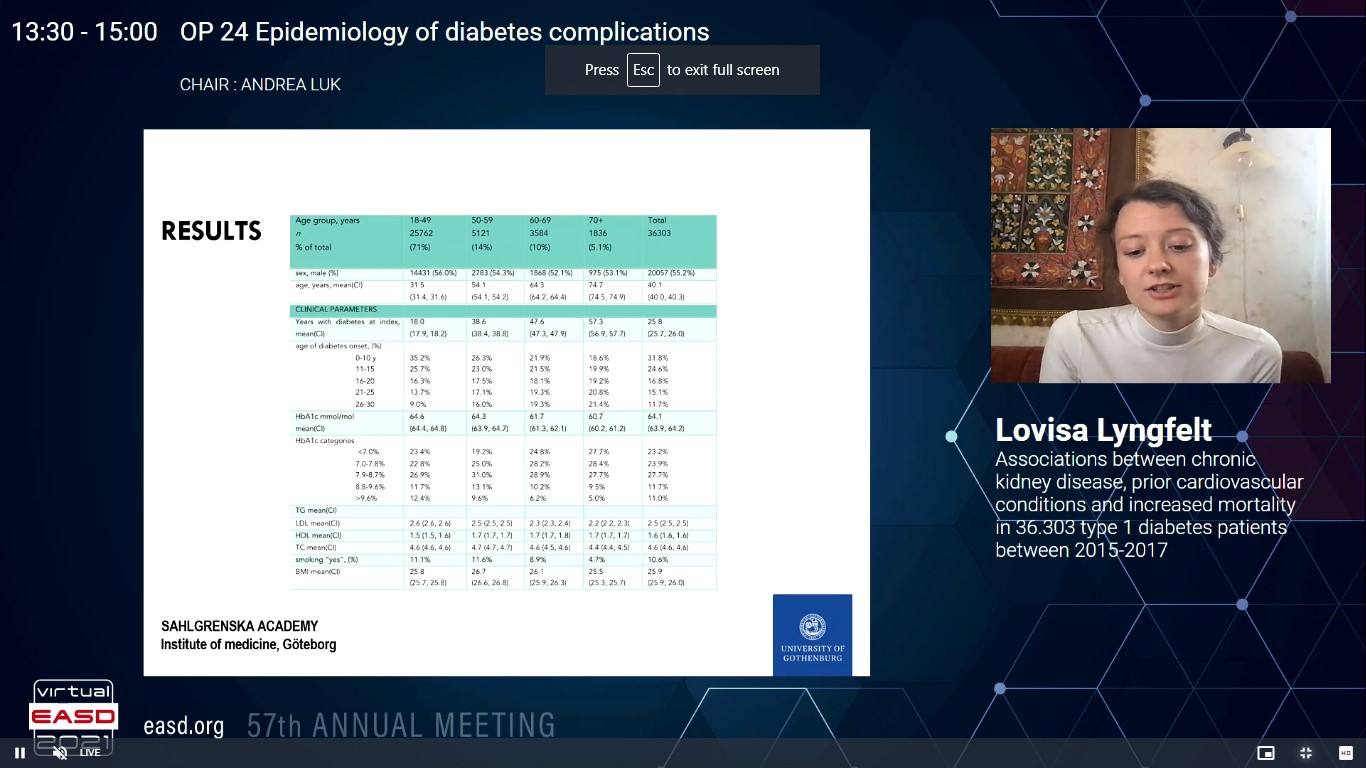
People with type 1 diabetes (T1D) yet have an increased risk of premature death than the general population, generally due to cardiovascular disease. Lyngfelt L, presented a study in a session at Virtual EASD Annual Meeting 2021 on 29th September 2021 which explored updated information on the importance of previous heart failure, kidney disease, and atherosclerotic vascular disease for the risk of mortality in a nationwide, registry-based group of T1D.
All T1D patients (n=36 303) were included in the study from the Swedish National Diabetes Register (NDR) during the inclusion period between January 1, 2015 and December 31, 2017. NDR data were associated to data from various national health registries via each patient’s unique personal identification number. The cumulative mortality was explained by Kaplan-Meier curves, and analysed for correlation to prospective risk factors by a Multiple Cox regression model incorporating age, gender, diabetes duration, HbA1c, BMI, SBP, DBP, albuminuria, previous cardiovascular disease (CVD), coronary heart disease, acute myocardial infarction or stroke, heart failure (HF) and eGFR stage as independent parameters.
Mean age at index day was 40.1 years, 55% were men and mean duration of diabetes was 25.8 years. Record of previous CVD, was shown in 8.7%, and prior HF in 1.7%. Normal kidney function (chronic kidney disease (CKD) stage G1; eGFR ≥90) was exhibited in 50%, and 70% were normoalbuminuric. The mean follow-up time was 3.3 years with a minimum patient follow-up time of 1 year. Total 1127 patients were died with an observed crude total mortality rate of 0.92 deaths/person year. In multivariate analysis, the risk in all-cause mortality was HR (hazard ratio) 1.91 (95% CI 1.66-2.20) in patients with prior CVD as compared to persons free of CVD at baseline. In patients with HF adjusted HR was 1.92 (1.66-2.23). Patients with impaired kidney function (moderate, high and very high CKD stages) showed HR 1.47 (1.19-1.80), 2.78 (2.11-3.66), and 3.80 (2.80-5.16), respectively, in multivariate analysis. The cumulative mortality for people with T1D and varying degrees of CKD, were shown with and without previous CVD and HF.
In the registry-based observational study, a previous history of CVD, HF, and CKD all were correlated with an elevated risk of death, and a combination of risk conditions with significantly increased risk for patients with T1D.
Heart failure and Renal Complications in Young- and Usual-onset Type 2 Diabetes among White Caucasians from US and UK
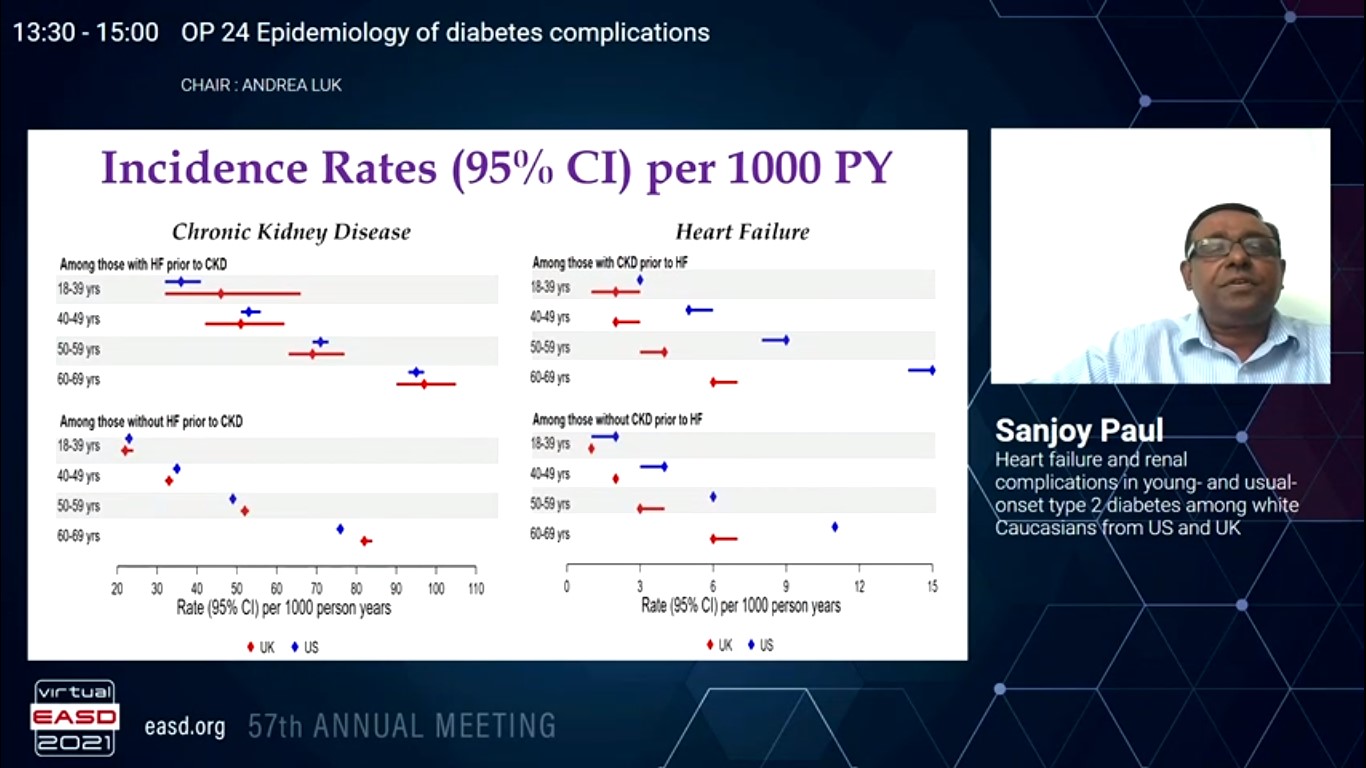
Although people with T2DM are well known to have elevated risk of chronic kidney disease (CKD) and heart failure (HF), the population-level evidence on the risk of these incidents in young- and usual-onset T2DM in various healthcare setups is deficient. Paul S, presented a study in a session at Virtual EASD Annual Meeting 2021 on 29th September 2021 which analysed the risk of CKD and/or HF in White Caucasians with T2DM in two different healthcare setups following the same study design. The prospective difference in risk dynamics among male and female over age groups were also analysed.
1491672 and 103233 White Caucasians diagnosed with T2DM among 2000 and 2018 in the age groups of 18-39 /40-49 / 50-59/ 60-69 years were recognized with nationally representative electronic medical records of US and UK. Date of T2DM diagnosis was contemplated as baseline, with first date of CKD or HF diagnosis (CKDHF) or end of follow-up from baseline contemplated as the time to incident. The risk of CKDHF (hospitalisation or physician coded events) was assessed in males and females in different age groups adjusting for time-differing covariates. Adjusted mean time to CKDHF was measured by a propensity score based modelling approach, balancing and adjusting for confounders.
50 /59% were male, 10 /13% showed CKD, 2 /2% showed HF, 48 /55% with hypertension, 39 /31% with dyslipidaemia, 13/15% with cardiovascular disease, and 20 /15% with microvascular disease at T2DM dx in US /UK. 24 /9% were on insulin and 34 /33% exhibited depression prior to CKDHF or end of follow-up. 95% CIs for incidence rates per 1000PY for CKDHF were: (23-24) /(22-24) in 18-39 years, (37-38) /(33-35) in 40-49 years, (53-54) /(53-55) in 50-59 years and (82-83) /(83-86) in 60-69 years in US /UK with mean 4.9-5.1 /7.3-7.5 years of follow-up across all age groups in US /UK. In the youngest age group in US /UK, male showed substantially greater CKDHF rate and 25% (HR CI: 1.20-1.29) /31% (HR CI: 1.14-1.53) greater adjusted risk as compared to female. But, in the 50+ year groups, male showed substantially lower rate and 3-11 / 21-23% lower risk [range of HR CI: 0.88-0.98 /0.73-0.82] as compared to female in US /UK. Adjusted years (CI) to CKDHF in 18-39 years group were 9.7 (9.2, 10.2) /8.9 (8.0, 9.7) in US/UK, only 4.2 / 2.6 years later compared to 5.5 (5.4, 5.6) /6.3 (6.2, 6.5) years in 60-69 years group. The time to event(s) was similar within age groups < 60 years in US and UK.
Although healthcare systems vary over countries, White Caucasian males and females with young- and usual-onset T2DM showed similar risk paradigm for CKD and HF. This clearly recommends a frequent global approach in the proactive treatment of macro- and microvascular risk concurrently in people with T2DM, especially between young-onset T2DM who progress CKD or HF only 3-4 years later as compared to the usual-onset.
Characteristics and Predictors of Mortality in Diabetes Patients Hospitalised with COVID-19: A Single-centre Cohort Study from Poland
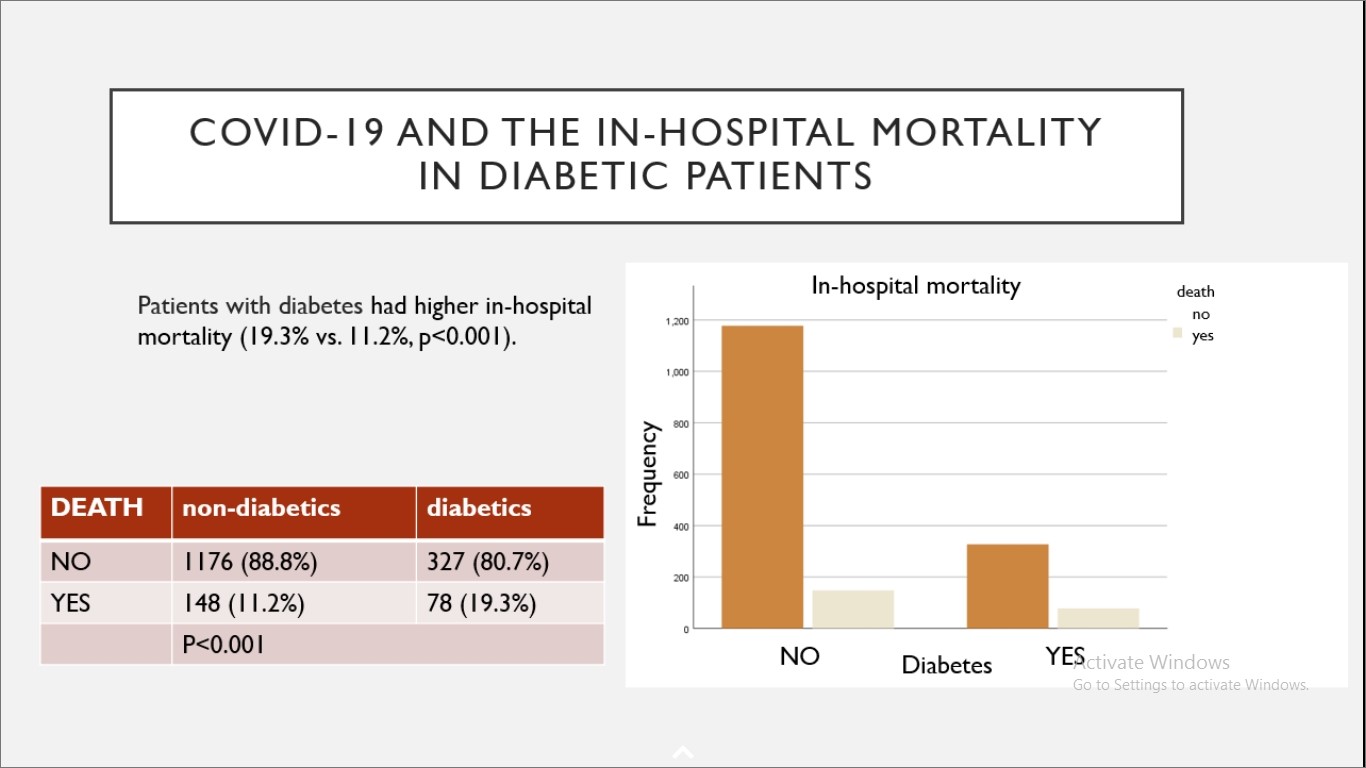
COVID-19 was detected in more than 25 million people in the European Union, and more than 2 million in Poland by the end of March 2021. Based on the previous studies, it is measured that 10-20% of these COVID patients also have diabetes. In the route of COVID-19, diabetes has been identified as a main risk factor for an admission to the intensive care unit, starting of mechanical ventilation and mortality. This is the first attempt of a large-scale examination of the course of COVID-19 in hospitalized patients with diabetes in Poland. Thus, Kania M, presented a study in a session at Virtual EASD Annual Meeting 2021 on 29th September 2021 which aimed to specifies the group of diabetic patients hospitalized because of the COVID-19 infection and recognize prospective factors correlated with unfavourable results.
The data was analysed retrospectively of a group of patients admitted because of COVID-19 to the University Hospital in Cracow, Poland from March 6 and October 15 2020. Data was gathered from electronic patients’ records regarding their basic clinical and biochemical variables, therapies and results. Their basic characteristics and predictors of hospital mortality were analysed.
1729 patients from the studied period were included. 23.3% (404 patients) patients showed diabetic prevalence. Diabetic patients were older as compared to the non-diabetic group (median age 71 years, p<0.001), with similar gender distribution (males: 53.8% vs. 50.5%, p=0.24). Patients with diabetes showed longer hospital stay (medians: 18 vs. 16 days, p<0.001), needed more commonly admission into an ICU (16.5% vs. 9.7%, p<0.001), mechanical ventilation (12.1% vs. 8%, p=0.011), and showed greater mortality (19.3% vs. 11.2%, p<0.001). A multivariable logistic model was performed for predictors of mortality. The model incorporated the following parameters – age, sex, glycemia over 10 mmol/l, C-reactive-protein (CRP) level and white blood cells count on admission, history of hypertension, heart failure, ischemic heart disease, inhospital use of dexaven, antiplatelet drugs, anticoagulation therapy, ACEI/sartan, statin, metformin and insulin. Three parameters – older age, higher CRP and dexaven use – were correlated with a higher death rate (OR 1.795%CI 1.03-1.11; 1,005 95%CI 1.001-1.01 and 2.32 95%CI 1.013-5.33 respectively), while metformin use was correlated with lower mortality (OR0.22 95%CI 0.9-0.55).
Diabetes was exhibited in about one fourth of hospitalized patients in the setting. This group of patients with diabetes showed nearly twice as high mortality as compared to non-diabetics. Older age and markers of high inflammatory reactions were recognized as risk factors for mortality.
The Impact of Acute-to-chronic Glycaemic Ratio as a Predictor of COVID-19 Severity and Mortality
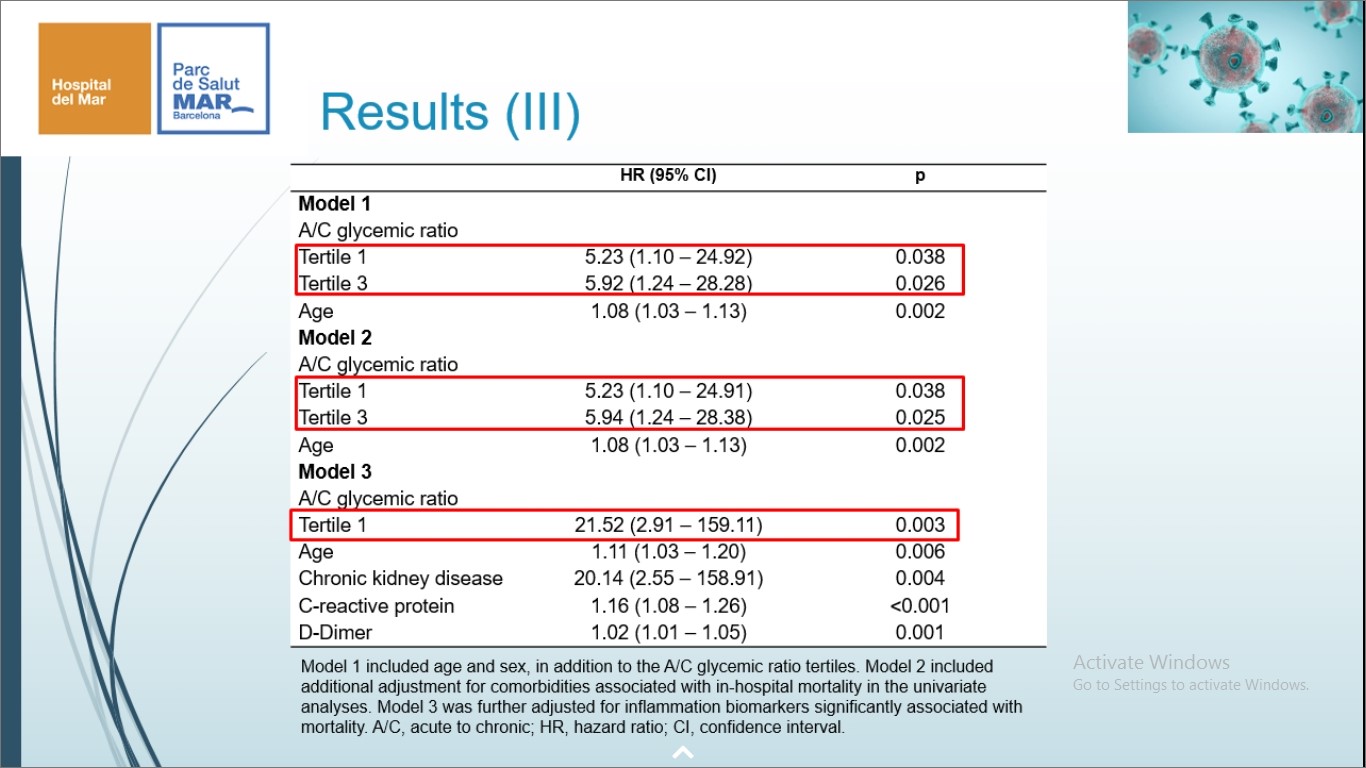
Underlying diabetes mellitus (DM) has been contemplated a risk factor for elevated COVID-19 extremity and worse results, incorporating higher mortality. But, no previous studies have evaluated whether the combined analysis of acute and chronic glycaemic levels may have a superior prognostic value than each component alone. Ramon J, presented a study in a session at Virtual EASD Annual Meeting 2021 on 29th September 2021 which assessed whether the acute-to-chronic glycaemic ratio (ACR) was correlated with mortality and extreme effects in patients with DM hospitalized for COVID-19.
All patients with DM hospitalized for COVID-19 among March 2020 and May 2020 was registered in an observational cohort study. Demographic and clinical data were gathered, incorporating data on clinical treatment, analytical variables, glycaemic control (glycaemia at admission, HbA1c) and inflammatory markers, extremity scales (MEWS, CURB65) and severity outcomes (length of hospital stay, intensive care unit (ICU) admission, acute respiratory distress syndrome (ARDS), invasive mechanical ventilation (IMV) and mortality. The formula eCGL= (28.7xHbA1c(%))-46.7 was used to measure the chronic glucose levels (CGL) . The ACR (glycaemia at admission/eCGL) were estimated for all patients.
A total of 91 patients were incorporated. Baseline characteristics of the subjects were distinguished for ACR tertiles. Patients in the 3 tertile showed greater glucose levels upon admission and higher concentrations of inflammatory markers. A glucose level at admission >200mg/dL was correlated with ARDS (OR=3.8 (1.4-10.2); p=0.008), IMV (OR=8.6 (1.8-41.5); p=0.008) and ICU admission (OR=9.4 (1.9-45.1); p=0.005) however was not correlated with the length of stay or mortality. By contrast, a Ushape curve correlation was found among the ACR tertiles and mortality. The 1 ACR tertile exhibited a trend towards greater mortality (OR=4.9 (0.9-25.2); p=0.059) and the 3 ACR tertile was substantially correlated with greater mortality (OR=6.0 (1.2-30.7); p=0.032) than the 2 tertile.
The ACR showed a U shaped mortality curve in patients with underlying diabetes. These findings recommend that an unbalance among the acute glycaemia at admission and the chronic metabolic control exhibited greater mortality rates, adding a superior prognostic value than each component alone. By difference, hyperglycaemia at admission was correlated with a greater inflammation status and poor extremity results.
Inside CKD: Modelling the Clinical and Economic Impact of Routine Screening for Albuminuria in People with Type 2 Diabetes

In patients with type 2 diabetes (T2D), early detection of chronic kidney disease (CKD) followed by guideline-recommended interventions is key to slowing CKD development; however adherence to screening recommendations is negligible. Inside CKD models the global burden of CKD by country-specific, patient-level microsimulation models. Power A, presented a study in a session at Virtual EASD Annual Meeting 2021 on 29th September 2021 which modelled the impacts of targeted implementation of urine albumin:creatinine ratio (UACR) estimation and interference in patients with T2D.
The Inside CKD microsimulation was used to model the effect of estimating UACR in routine primary care visits with consecutive intervention in patients with T2D aged ≥ 45 years with a range of kidney functions as compared to current practice. Published country-specific data on demographics, CKD (albuminuria and estimated glomerular filtration rate status), T2D, comorbidities and complications was used to construct the virtual populations.
Preliminary data for 3 countries exhibited that the estimation of UACR with conscutive intervention in patients with T2D would inhibit CKD development to stages 3b to 5 in 164 739 patients in the UK, 964 121 in the US and 156 482 in Canada from 2020 to 2026. correlated cost savings would be £0.14B, US$13.81B and C$2.34B. Furthermore countries will be examined.
Routine UACR estimation with consecutive intervention could prospectively decrease the global burden of CKD and healthcare costs in patients with T2D and enhance patient results.
