Taubel J. Eur Heart J. 2021 Jan 7;42(2):178-188.
The microRNA-132-3p (miR-132) is a regulatory (noncoding) RNA which is upregulated in cardiac tissue in response to cardiomyocyte stress. Preclinical studies exhibited miR-132 to impact signalling pathways included in cardiomyocyte growth, autophagy, calcium handling, and contractility. Over-activation of miR-132 in cardiac tissue increases adverse cardiac remodelling causes hear failure (HF). A first-in-class miR-132 inhibitor was CDR132L, a synthetic locked nucleic acid antisense oligonucleotide (ASO) inhibitor with a fully phosphorylated backbone. The promising preclinical remarks and the detailed toxicological profile of ASOs move to conduct this first-in-human study straight in patients with stable chronic HF of ischaemic origin. Taubel J, et al., conducted a clinical Phase 1b study to analyse safety, pharmacokinetics, target engagement, and exploratory pharmacodynamic impacts of CDR132L in patients on standard-of-care treatment for chronic ischaemic HF.
This First‐in‐human (FIH) Phase 1b, prospective, randomized, double-blind, placebo-controlled, dose-ranging study of intravenous CDR132L was executed from June 2019 to March 2020. Patients 30– 80 years old were enrolled in the study with New York Heart Association class 1–3 chronic HF with left ventricular ejection fraction (LVEF) between ≥30% and <50% or N-terminal pro b-type natriuretic peptide (NT-pro BNP) >125 ng/L at screening, and the body mass index of 18–28 kg/m2. Patients endured on guideline-directed standard-of-care treatment for HF, and on stable medication for comorbidities. Patients were randomized 5:2 to CDR132L or placebo (0.9% saline). For each patient, 4 months was the overall study period. All patients underwent physical examination, vital signs, standard haematology, biochemistry, and coagulation ascertains at prespecified time points all over the study. A comprehensive echocardiographic analysis, incorporating LVEF determination, was executed at screening, baseline, and Days 56 and 112 to analyse the safety and explore pharmacodynamics of CDR132L. Additionally, HF relevant blood biomarker were evaluated at prespecified time points. Holter electrocardiograms (24 hr) were recorded at screening, 12-lead real-time electrocardiograms (continuous telemetry), from 1 h pre-dose to 24 hr post-dose, and further 12-lead resting electrocardiograms at time points matching pharmacokinetic/pharmacodynamic sampling. The primary outcome was safety analysed in terms of treatment emergent adverse events (TEAE) and change in laboratory values, while the secondary outcome was pharmacokinetic profiles for single and repeated ascending CDR132L doses.
A total of 116 patients with HF were screened. 28 patients shown eligibility criteria, of whom 20 patients were randomized to CDR132L and 8 patients to placebo. All patients finished the study as planned. Treatment was safe and well tolerated with CDR132L, 0.32–10mg/kg. Thrombocytopenia, pre-specified as a prospective adverse event of special interest (AESI) was not observed because of experience with certain first-generation ASOs. Platelet counts lasted normal and stable all-over. High-sensitivity troponin T concentration which is observed as a safety marker of ischaemic injury showed no clinically substantial changes from baseline values (Figure 1).
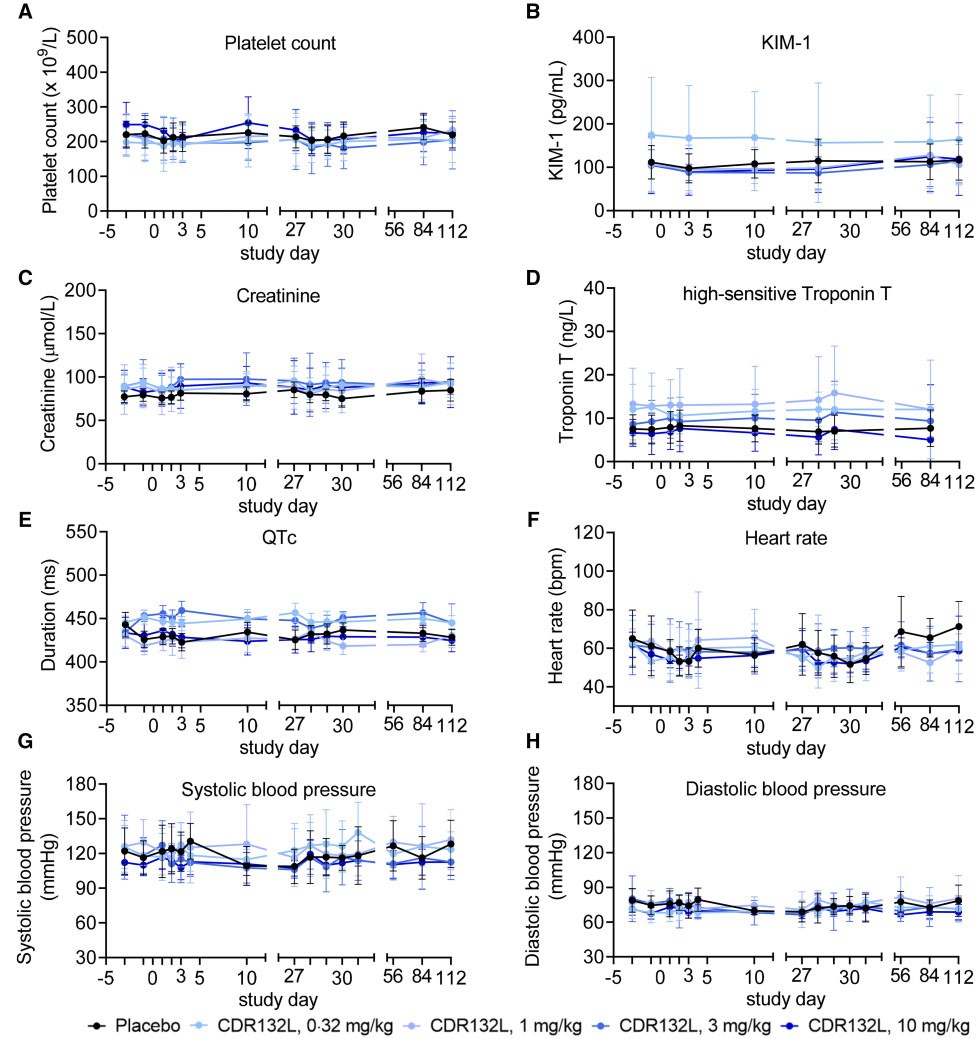
Figure 1: Selected safety variables over time. Data are mean (95% confidence interval).
CDR132L exposure was compatible from Days 1 and 28 administrations (Figure 2), and intra-patient variability was mainly within the expected physiological norm (<30%).
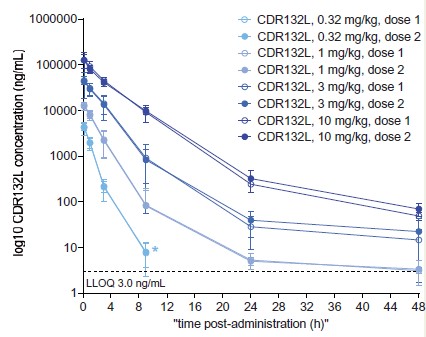
Figure 2: Plasma CDR132L concentrations through 48 h after CDR132L administrations.
Data are mean (95% confidence interval). Measurements were taken 9min and 1, 3, 9, 24, and 48 h after CDR132L administration. *CDR132L concentration fell below the lower limit of quantification at subsequent time points.
CDR132L administration showed rapid, sustained and sharp decrease in plasma miR-132 mainly at higher dose levels ≥1mg/kg, in the 4-month course of the study (Figure 3A). Patients managed with 3 or 10mg/kg CDR132L exhibited sustained low plasma miR-132 levels similar to the range in healthy volunteers (median level: 0.0004) (Figure 3B).
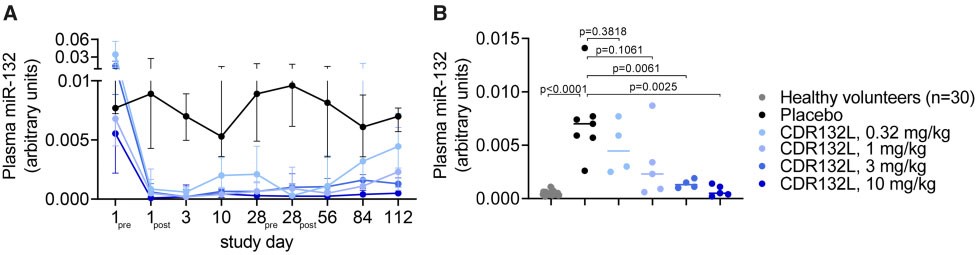
Figure 3: Plasma miR-132 levels in patients after CDR132L treatment.
(A) Median with 25%/75% interquartile ranges of plasma miR-132 levels in patients over the study course (pre = immediately before, post = 1h after administration). (B) Individual median miR-132 levels in healthy subjects (n= 30; blood bank samples) and in patients (n= 25) at study end (Day 112). p-value: Mann–Whitney U test comparing to the placebo group.
Thus, it was concluded that this study is the first clinical trial of HF patients with an antisense medication. CDR132L was prudent and well tolerated, verified linear plasma pharmacokinetics with no symptoms of aggregation, and recommends cardiac functional enhancements.
